Laryngomalacia in infants: when to treat

Breathing problems
Infant and newborn care
Laryngomalacia is the most common cause of stridor in infants. It is caused by collapse of the tissues above the vocal cords on inspiration. Surgical intervention may be required to manage failure to thrive, respiratory distress or sleep apnoea.
- Laryngomalacia is the most common cause of infantile airway noise, usually becoming prominent in the first few weeks of life.
- The hallmark symptom of high-pitched inspiratory stridor helps to differentiate laryngomalacia from other airway conditions.
- There is a spectrum of severity, but many cases of laryngomalacia are mild and resolve spontaneously by 2 years of age.
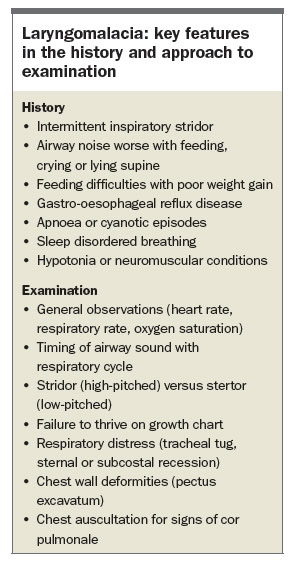
- Severity is determined by the presence of feeding difficulties, poor weight gain, respiratory compromise, hypoxia or hypercapnia, aspiration, cyanotic episodes, apnoea and cor pulmonale.
- Weighing the child regularly to monitor growth, supportive management to improve feeding, and acid suppression therapy for concurrent symptoms of gastro-oesophageal reflux disease may be of benefit as initial steps.
- The patient should be referred to an ENT surgeon if there are obstructive airway symptoms, failure to thrive or any other parental concerns. A fibre-optic examination performed in the office can confirm the diagnosis of laryngomalacia and the need for further investigation or intervention with supraglottoplasty.
Picture credit: © Blend/Ariel Skelley/Medical Images Models used for illustrative purposes only
Laryngomalacia is the most common congenital laryngeal anomaly, accounting for 60 to 70% of stridor in neonates and infants.1 Infants typically present with inspiratory stridor in the first few weeks of life, with a very small proportion having airway noise from birth. The symptoms may increase over the first 6 to 8 months of life but usually abate gradually and resolve by the age of 18 to 24 months. Many cases are mild and do not require investigation or treatment.
In laryngomalacia, collapse of the tissues above the vocal cords causes airway obstruction on inspiration. There are several theories about why this occurs, but poor laryngeal tone in association with neuromuscular inco-ordination is the most likely cause.2 A relationship with gastro-oesophageal reflux disease (GORD) has been noted but not fully elucidated, although GORD is thought to irritate the laryngeal tissues and affect the sensorimotor integration of vagal responses.3
Clinical features
Parents may present with concern about an infant who makes unusual breathing noises at various times through the day and sometimes at night. They may note that other people have commented on the noise. A degree of parental anxiety about ‘my child stopping breathing’ is common.
The hallmark symptom of laryngomalacia is high-pitched inspiratory stridor, which is usually worse when the child is feeding, crying or lying supine. The noise may decrease when the child is settled or asleep.
Feeding difficulties are common, as the child may have trouble co-ordinating the suck–swallow–breathe sequence because of the intermittent airway obstruction. This can manifest as coughing, choking, regurgitation and slow feeding. Associated symptoms of GORD may be exacerbated by the negative inspiratory pressures generated to breathe past the obstruction. Weight gain can be affected, particularly if great respiratory effort is required, coupled with poor caloric intake.
In some circumstances, the infant may have apnoeic episodes, when awake or asleep, which should alert the clinician to refer the patient to an ENT surgeon for urgent review The presence of a neuromuscular disorder or hypotonia may predispose a child to a variant of laryngomalacia that is less responsive to standard management options.
When examining an infant with noisy breathing, time should be taken to observe the child when awake, agitated, asleep and feeding. Attention should be paid to the nature of the sound: high-pitched stridor arises from the laryngeal region, whereas low-pitched stertor (like a snoring sound) tends to arise from the postnasal and pharyngeal regions. A stethoscope placed at the neck can help to distinguish the phase of respiration in which the noise is loudest: the inspiratory phase indicates a supralaryngeal or laryngeal anomaly, whereas the expiratory phase indicates a lower airway anomaly (e.g. asthmatic wheeze). It is useful to ask parents if they have video recordings of the child exhibiting the airway noise or any episodes of concern, as the symptoms can be intermittent and may not be severe at the time of consultation. The child should be weighed bare and the weight plotted on the growth chart to detect any failure to thrive. Signs of work of breathing include tachypnoea, tracheal tug and sternal or subcostal recession. Pectus excavatum may be present.
Baseline oxygen saturation level in room air can be useful to guide assessment of the degree of severity of laryngomalacia.4 Moderate and severe cases may be associated with reduced oxygen saturation levels. However, a normal oxygen saturation level should not falsely reassure the practitioner if the clinical symptoms are concerning. The nose and oral cavity should be examined to exclude other causes of upper airway obstruction. Chest auscultation is important as there may be signs of cor pulmonale in severe cases (Box).
{kind=link}
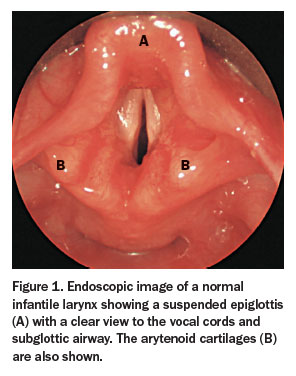
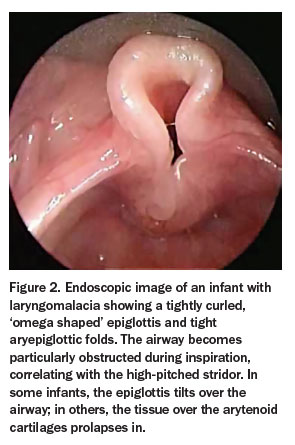
The features of a normal infantile larynx and those of a larynx affected by laryngomalacia are shown in Figures 1 and 2, respectively. Laryngomalacia has various appearances, including the tightly curled, ‘omega shaped’ epiglottis, short aryepiglottic folds and prolapsing mucosa over the arytenoid cartilages during inspiration. The different anatomical variants all result in the same high-pitched airway noise.
{kind=link}
{kind=link}
Differential diagnoses
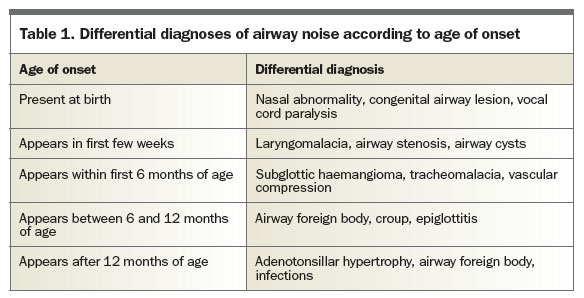
There are many other conditions that can cause airway noise in an infant. The onset of the sound, its nature and associated symptoms can help to differentiate laryngomalacia from other abnormalities (Table 1). For example:
{kind=link}
- a noise present from birth may indicate a congenital anomaly, such as vocal cord paralysis
- a noise that starts in the first few months of life associated with a cutaneous haemangioma in the facial region could indicate a subglottic haemangioma
- the presence of other upper respiratory symptoms and fever could point towards croup, bacterial tracheitis or even epiglottitis
- the sudden onset of an airway noise in an older infant who can crawl and pick up items may be caused by unwitnessed inhalation of a foreign body.
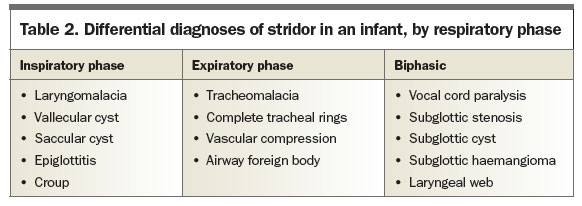
Paying attention to the phase of respiration in which stridor occurs can guide towards alternative diagnoses (Table 2), although it can be difficult to make a definitive diagnosis at the bedside, even for a clinician with an experienced ear.
{kind=link}
Initial management
Laryngomalacia can be classified as mild, moderate or severe. Severity depends on feeding and obstructive symptoms rather than the degree of airway noise. Mild and moderate cases each account for about 40%. Severe cases account for the remaining 20% and are more likely to require surgical intervention.3 Determining the severity assists with primary care management and need for referral.
In mild cases, the noise is usually not concerning, feeding is minimally affected and the infant is generally thriving appropriately. As the child grows, the stridor gradually becomes less frequent and less noticeable. It eventually disappears without intervention, although some infants may require treatment with an H2-receptor antagonist or proton pump inhibitor if there are concurrent symptoms of GORD. Acid suppression is more often required for moderate or severe cases of laryngomalacia, where the average duration of therapy is nine months.4 Regular GP review is important to ensure complete resolution over time.
Feeding difficulties are more prominent in children with laryngomalacia of moderate severity. These children can have trouble with choking and aspiration, work of breathing and slower weight gain. Feeding modification with pacing, upright position and texture modification may help alleviate these problems. Weekly monitoring of weight and provision of antireflux measures are often necessary. In some cases, if the child is having trouble with a co-ordinated swallow or aspiration or is not tracking well on the growth charts, review by a speech therapist and supplemental nutritional support via a nasogastric tube can be considered. If there is concern about other anomalies, an x-ray of the lateral airways or chest is helpful. Baseline oxygen saturation levels may be lower than expected, in children with moderately severe laryngomalacia, and infants may experience apnoeic events warranting referral to an ENT surgeon.
As the severity progresses, the airway obstruction results in cyanotic episodes, apnoea and failure to thrive. The child may have an oxygen requirement, pectus excavatum deformity and, rarely, cor pulmonale; urgent hospital referral is essential in any of these circumstances.
When to refer
Any infant with airway noise that is persistent and of concern to the parents should be referred to an ENT surgeon, who can further examine the child’s upper airway with a flexible fibre-optic endoscope via the nose. This is a straightforward and safe procedure that can be performed in the office setting and allows the ENT surgeon to dynamically assess the larynx during respiration and to screen for other diagnoses. There is also the option of diagnostic laryngo-broncho-oeosophagoscopy to formally examine the airway structures under general anaesthesia.
As infants with moderate or severe cases of laryngomalacia may require surgical intervention with a supraglottoplasty, these children should be referred to an ENT surgeon for assessment. A subset of infants with laryngomalacia who have symptoms predominantly when asleep may benefit from review by a sleep medicine specialist, for consideration of overnight oximetry or full polysomnography testing, if appropriate.
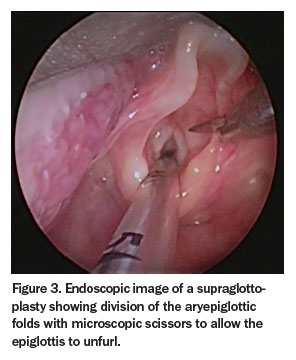
A supraglottoplasty, when required, is directed towards the patient’s specific anatomical deformity. Tight aryepiglottic folds can be released, excess prolapsing mucosa can be excised, and the epiglottis can be sutured to prevent it prolapsing (Figure 3). Postoperative monitoring for bleeding or oxygen desaturation is important but, in general, most patients recover quickly and the procedure has a success rate of about 90%.1 Aspiration is an uncommon but feared risk and is more likely in children with hypotonia or neurological comorbidity.5 Revision surgery may be required (in 3 to 9% of patients) if symptoms progress or fail to resolve.5
{kind=link}
Even though surgery can alleviate obstructive symptoms and improve oral intake, the natural history is for the stridor to disappear gradually over many months. Despite reports of some patients having occasional symptoms related to sleep, exercise and feeding in later childhood, parents can be confidently reassured that in most children the condition will completely resolve well before then, without any long-term effects.RMT
References
- Dobbie AM, White DR. Laryngomalacia. Pediatr Clin North Am 2013; 60: 893-902.
- Munson PD, Saad AG, El-Jamal SM, Dai Y, Bower CM, Richter GT. Submucosal nerve hypertrophy in laryngomalacia. Laryngoscope 2011; 121: 627-629.
- Landry AM, Thompson DM. Laryngomalacia: disease presentation, spectrum, and management. Int J Pediatr 2012; 2012: 753526.
- Thompson DM. Laryngomalacia: factors that influence disease severity and outcomes of management. Curr Opin Otolaryngol Head Neck Surg 2010; 18: 564-570.
- Denoyelle F, Mondain M, Gresillon N, Roger G, Chaudre F, Garabedian EN. Failures and complications of supraglottoplasty in children. Arch Otolaryngol Head Neck Surg 2003; 129: 1077-1080.