Bronchoscopic procedures for COPD: a breath of fresh air

COPD (chronic obstructive pulmonary disease)
Lung diseases
Chronic obstructive pulmonary disease affects about 15% of the Australian population aged over 40 years and 40% of those aged over 75 years. Treatment options for advanced disease are limited, but novel bronchoscopic procedures can offer physiological benefits in carefully selected patients.
Chronic obstructive pulmonary disease (COPD) is a chronic lung condition characterised by airflow obstruction that is not fully reversible. It is a progressive disease that results from an inflammatory response in the lungs to noxious environmental stimuli such as cigarette smoke most commonly but also biofuel mass exposure, air pollution and occupational fumes and dusts. COPD is an umbrella term for the two areas of the lung affected by these toxins: the airways, resulting in chronic bronchitis, and the lung parenchyma, resulting in emphysema.
COPD: its impact
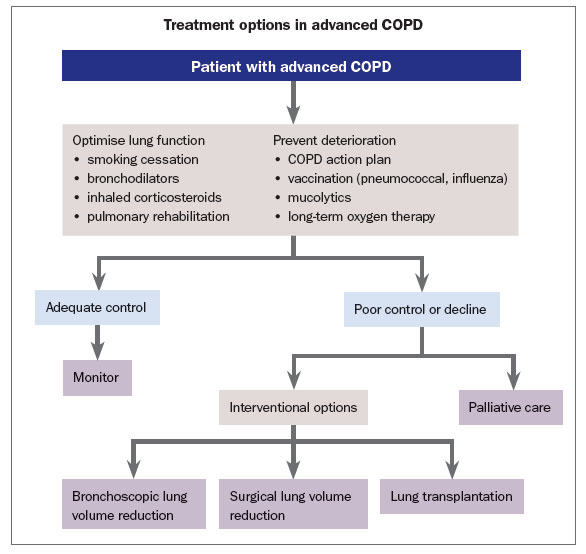
COPD affects nearly 15% of the Australian population aged over 40 years and 40% of those aged 75 years and over, with about 2% of people in this older age-group having advanced disease (GOLD Stages III or IV).1 COPD was the fifth leading cause of death in Australia in 2013, with an economic cost estimated at 8.8 billion dollars.2,3 GPs in Australia have ready access to the COPD-X guidelines for case finding, diagnosis, management and optimising quality of life in patients with COPD across all stages of severity.4 These guidelines offer a comprehensive armamentarium of both pharmacological and nonpharmacological strategies to optimise function and to prevent and manage COPD exacerbations (Flowchart). However, despite best practice, many patients with advanced COPD continue to experience debilitating symptoms.
{kind=link}
Surgical treatment for COPD
Surgical treatment for advanced disease (surgical lung volume reduction) showed promise in the 1990s but a randomised trial comparing this with best medical care showed only small subgroups of patients benefited, and the associated high morbidity and mortality led to its abandonment in most centres.5 Lung transplantation offers a reprieve for only a small minority of sufferers; in 2015 there were 195 lung transplant recipients in Australia, only a third of whom had COPD.6
Bronchoscopy and COPD
Bronchoscopy is a minimally invasive way of accessing the lungs using a flexible videobronchoscope. Usual indications include diagnosis and staging of lung cancer, evaluation of haemoptysis and sampling airway secretions for infections. More recently, bronchoscopy has moved to the next level with novel techniques for lung biopsy, for sampling solitary pulmonary nodules and for palliating symptoms of obstructing lung cancers with stents, lasers, snares and cryoprobes.
In the last decade, techniques have been developed for treating patients with advanced COPD aiming to achieve the same physiological benefits noted with lung volume reduction surgery but without the complications and prolonged convalescence associated with a major operation. International COPD guidelines now recommend consideration of bronchoscopic therapies in carefully selected patients.7
How does lung volume reduction help patients with COPD?
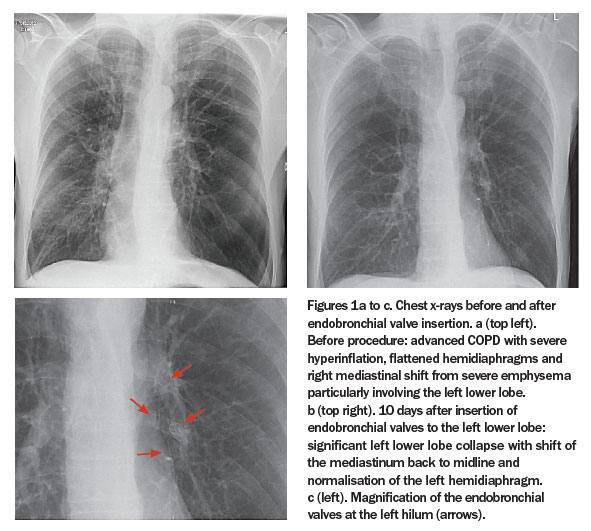
Severe emphysema is characterised by the formation of blebs and bullae beyond the terminal bronchi. Emphysematous lung not only fails to contribute to gas exchange but the resultant gas trapping and hyperinflation compresses less affected lung, expands the chest wall and flattens the hemidiaphragms further impairing breathing mechanics (Figure 1). Surgical lung volume reduction removes the most severely affected emphysematous lung by resection, reversing this pathophysiology.
{kind=link}
The aim of bronchoscopic lung volume reduction is to collapse, rather than resect, the emphysematous lung and thus avoid the complications of a sternotomy or thoracotomy. The benefits of lung volume reduction include improved chest wall and diaphragm biomechanics, increased lung elastic recoil and better matching of ventilation and perfusion.8 These changes can lead to improvements in exercise capacity and ultimately quality of life.
What is bronchoscopic lung volume reduction?
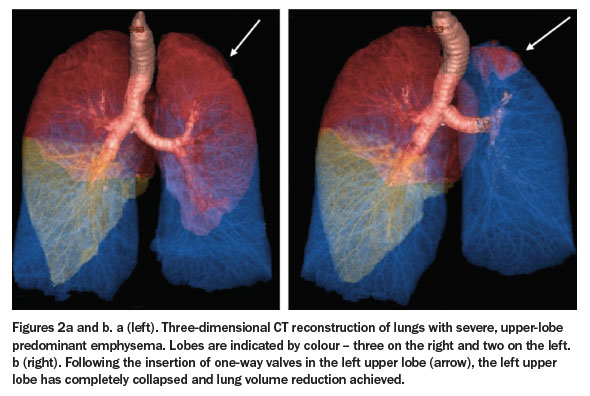
Several techniques have been developed to achieve bronchoscopic lung volume reduction (BLVR). Most often in Australia, one-way valves are inserted via the working channel of a bronchoscope to block the most emphysematous lobe. These valves allow expulsion of air and mucus from the lobe during expiration and prevent air re-entering during inspiration, resulting in progressive atelectasis and collapse over several hours to days (Figures 1b and c and Figure 2).
{kind=link}
Typically, three to six valves are required to block a whole lobe in a procedure that takes around 15 to 40 minutes. Insertion is usually performed under general anaesthesia but can be done under conscious sedation.
Anatomical considerations
The key to achieving volume reduction is ensuring that the target lobe is anatomically isolated from its adjacent lobe(s) to prevent air bypassing the valves and keeping the target lobe inflated, a process known as collateral ventilation. About half the general population have partially deficient, interlobar fissures (thin membranes that anatomically separate the lobes of each lung) and in these patients BLVR is unlikely to work. It is crucial therefore to select patients with no collateral ventilation.
Collateral ventilation can be assessed in two ways. The first is by inspecting the interlobar fissures on high-resolution chest CT scans to ensure they are visible along their course (Figures 3a and b). The second is during bronchoscopy using a specially designed catheter (CHARTIS system) that assesses residual flow in a targeted lobe following occlusion of that lobe by an inflated balloon. If flow persists, collateral ventilation is likely to be present, whereas if flow gradually diminishes and stops, collateral ventilation is likely absent.
{kind=link}
What are the expected outcomes?
Several high-quality randomised controlled studies of BLVR in patients with advanced COPD have shown improvements in lung function, respiratory-related quality of life and exercise capacity.9-11 These studies have confirmed unequivocally that treatment responders are those who achieve lobar collapse after treatment, that is, patients with no collateral ventilation. This adds weight to the importance of case selection.
Although early valve studies accepted all patients with COPD and therefore showed only modest overall outcome benefits,12 recent studies in better selected patients show mean forced expiratory volume in 1 second (FEV1) improvements in the order of 20% or higher, increases in six-minute walk distance and clinically relevant improvements in quality of life scores. In our experience and in terms meaningful to our patients, we see patients returning to gardening, shopping independently and, in many cases, having reduced requirements for supplemental oxygen.
What are the complications?
The most common complications of BLVR are pneumothorax (occurring in 8 to 25% of patients), pneumonia (in up to 8%), acute exacerbation of COPD (in 12 to 22%) and valve migration (in 5 to 16%). 9-11
Pneumothorax
Pneumothoraces usually occur within two to three days of BLVR and are managed according to size and clinical consequence. Smaller pneumothoraces may be observed , but those that are larger or symptomatic require chest tube insertion, sometimes urgently. In the small minority where air leak persists beyond a week, one or more valves may require removal, but can be reinserted a few weeks down the track.
Pneumonia and COPD exacerbations
The use of periprocedural prophylactic antibiotics aims to reduce the incidence of acute pneumonia. Any patient with severe COPD undergoing bronchoscopy can suffer an acute exacerbation and the rate is not thought to be increased with BLVR. These are managed in the standard way with antibiotics, bronchodilators, systemic corticosteroids and noninvasive ventilation when required.
Failure to achieve lobar collapse
Unfortunately, about one-third of patients, despite rigorous screening for collateral ventilation, fail to achieve lobar collapse following BLVR. Sometimes this is due to valve misplacement or dislodgement, and occasionally a valve may be expectorated. Repeat bronchoscopy at one month is suggested for patients failing to achieve lobar collapse.
Who would be suitable and when to refer?
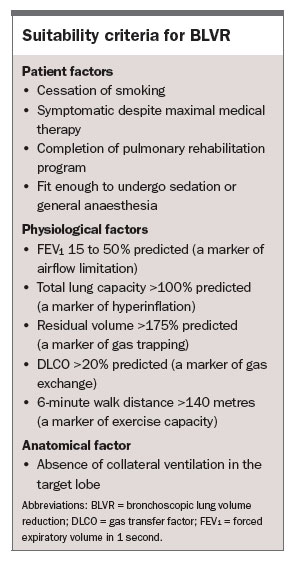
Appropriate patient selection is crucial for successful BLVR. In the first instance, patients must be optimally managed with evidenced based treatments. Australian COPD-X guidelines offer an excellent management resource.4 We would recommend that patients with COPD experiencing debilitating symptoms despite adherence to optimal therapy be referred to a lung specialist for assessment. Successful completion of a pulmonary rehabilitation program is highly desirable to ensure maximal fitness before the procedure. Being on home oxygen is not a contraindication but patients who are housebound or too unwell with comorbidities are probably too high risk to deal with general anaesthesia or complications such as pneumothorax.
Inclusion criteria for BLVR are divided into patient, physiological and anatomical factors (Box). Lung function parameters include severe airflow obstruction and high residual volume. The latter is a marker of gas trapping and strongly predicts treatment response. Anatomical factors are evaluated on high resolution CT scans of the chest and include regional emphysema scoring to help target the most affected lobe as well as fissure analysis using both automated software and direct visual assessment. Eligibility of patients should be discussed by a multidisciplinary team, including respiratory physicians, interventional pulmonologists, radiologists and thoracic surgeons.13
{kind=link}
What’s on the horizon for bronchoscopic COPD therapies?
Aside from using valves, several other techniques to achieve lung volume reduction are being evaluated across Europe, the USA and here in Australia, mostly in the setting of clinical trials. Examples include the use of steam or biological glue sealant directed into a target lobe to achieve lung volume reduction or the insertion of nitinol coils (5 to 10 cm in length) into airway segments to tether the lung tissue and improve elastic recoil. Emerging therapies such as bronchial wall denervation to block muscarinic transmission leading to bronchodilation and reduced mucous hypersecretion are also being evaluated in clinical trials and may further add to the armamentarium of bronchoscopic options.
Conclusion
Novel bronchoscopic treatments for patients with advanced COPD are now available. In carefully selected patients, bronchoscopic lung volume reduction can offer improvements in lung function, exercise capacity and respiratory-related quality of life above and beyond maximal medical therapies. Appropriate patients should be considered for specialist referral to discuss suitability and options. RMT
References
- Toelle BG, Xuan W, Bird TE, et al. Respiratory symptoms and illness in older Australians. The burden of obstructive lung disease (BOLD) study. Med J Aust 2013; 198: 144-148.
- Australian Institute of Health and Welfare (AIHW) National Mortality Database (Table S1). Available at http://www.aihw.gov.au/deaths/leading-causes-of-death/ (accessed April 2017).
- Access Economics for the Australian Lung Foundation. Economic impact of COPD and cost effective solutions. Brisbane: Australian Lung Foundation; 2008.
- Yang IA, Dabscheck E, George J, et al. The COPD-X Plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease 2016. Version 2.46, June 2016.
- Fishman A, Martinez F, Naunheim K, et al. National Emphysema Treatment Trial Research Group. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med 2003; 348: 2059-2073.
- ANZOD Registry, 2016 Annual Report, Chapter 8: Lung donation. Australia and New Zealand Dialysis and Transplant Registry, Adelaide, Australia; 2016. Available at: http://www.anzdata.org.au (accessed April 2017).
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of COPD, 2017. Available at: http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd/ (accessed April 2017).
- Chung SC, Peters MJ, Emmett L, Ing AJ. Effect of unilateral endobronchial valve insertion on pulmonary ventilation and perfusion: a pilot study. Respirology 2010; 15: 1079-1083.
- Davey C, Zoumot Z, Jordan S, et al. Bronchoscopic lung volume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR-HIFi study): a randomised controlled trial. Lancet 2015; 386: 1066-1073.
- Klooster K, ten Hacken NHT, Hartman JE, et al. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med 2015; 373: 2325-2335.
- Valipour A, Slebos DJ, Herth F, et al. Endobronchial valve therapy in patients with homogeneous emphysema. Results from the IMPACT Study. Am J Respir Crit Care Med 2016; 194: 1073-1082.
- Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med 2010; 363: 1233-1244.
- Herth FJ, Slebos DJ, Slebos DJ. Endoscopic lung volume reduction: an expert panel recommendation. Respiration 2016; 19: 241-250.