Management of severe asthma: where are we now?

Breathing problems
A 77-year-old man with severe asthma and a previous history of smoking is under consideration for biologic therapy. He has had persistent, disabling asthma symptoms despite good adherence to high-dose inhaled corticosteroid and long-acting beta-agonist therapy for more than 12 months. Does he qualify for biologic therapy and where should we start?
- Severe asthma represents about 4% of all patients with asthma.
- Biologic add-on therapy can be beneficial to certain patients with uncontrolled severe asthma, but they should first have their treatment optimised and their comorbidities managed.
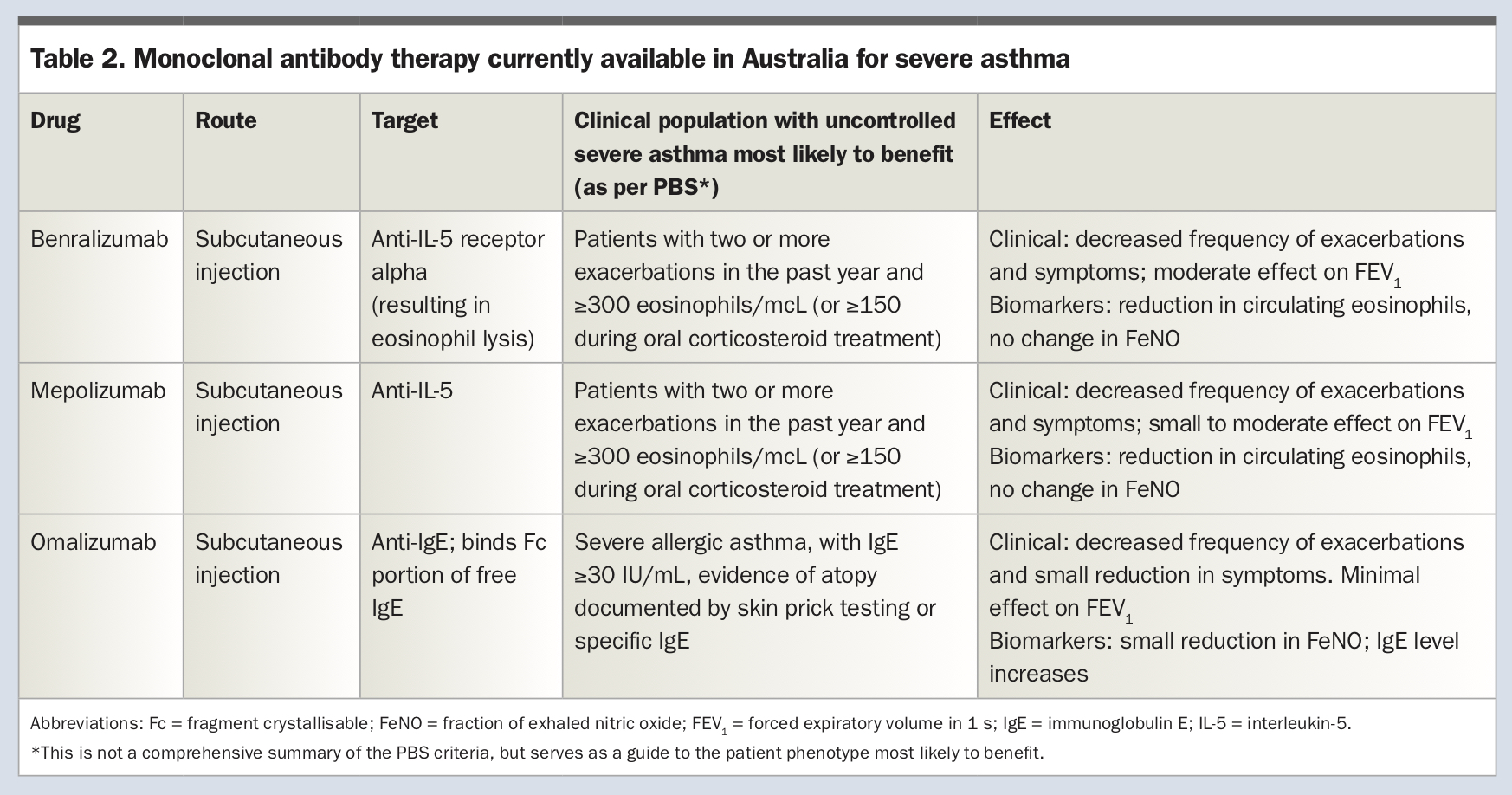
- Three biologics are currently approved for severe asthma phenotypes in adults and adolescents in Australia: mepolizumab (anti-interleukin [IL]-5 antibody) and benralizumab (anti-IL-5 receptor antibody) for severe eosinophilic asthma; and omalizumab (anti-immunoglobulin E) for severe allergic asthma.
- Recent PBS changes have removed some barriers to accessing these therapies.
Case scenario
Bill is a 77-year-old man with adult onset of frequent dyspnoea and wheeze that has significantly limited his activities in the past five years. He reports being very active as a child, playing football throughout his school years, and having no respiratory symptoms during childhood or adolescence. Bill began smoking cigarettes as a teenager and, by the time he successfully stopped smoking in his 50s, he had accumulated a 40 pack-year history of cigarette use. It was not until his late 60s that Bill began to experience episodic dyspnoea and wheeze, relieved by short-acting beta agonist therapy. In the 12 months before Bill’s referral to a specialist respiratory clinic, he was experiencing increasingly frequent respiratory symptoms that persisted despite prescription of an inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA) inhaler. Bill had never seen a respiratory physician and, given the frequent symptoms he was experiencing, his GP referred him to a specialist respiratory clinic for review.
Bill reports daily respiratory symptoms including breathlessness, chest tightness and wheeze, and on ‘bad days’ uses salbutamol nebulisers up to hourly. He says that initially he could still play football with his grandchildren without dyspnoea, but in the past 12 months, the frequency of his wheeze and dyspnoea means he is only able to walk very slowly. His usual 15-minute walk from his house to the local shopping centre can take him up to an hour now due to stopping to use salbutamol and to rest. He also wakes from sleep due to breathlessness more than once a week and has a persistent cough productive of a small amount of grey/white sputum. Bill identifies chocolate and exposure to strong perfumes as triggers for his breathlessness. He has a good sense of smell, denies any history of nasal polyposis, and has not had any adverse reactions to NSAID use. His other comorbidities include a fundoplication for gastro-oesophageal reflux disease (GORD), anxiety and chronic back pain.
Bill is now retired from working in a brewery, lives with his wife in Department of Housing accommodation and currently drinks minimal alcohol.
On examination at the respiratory clinic, there is an audible wheeze and Bill appears visibly breathless after walking less than 3 m. His oxygen saturation level is 98% on room air. There is no peripheral cyanosis or clubbing, no inflammation in the throat and no nasal polyps are visible. Examination of the chest after salbutamol administration reveals widespread expiratory and inspiratory rhonchi. His body mass index is 30.8 kg/m2.
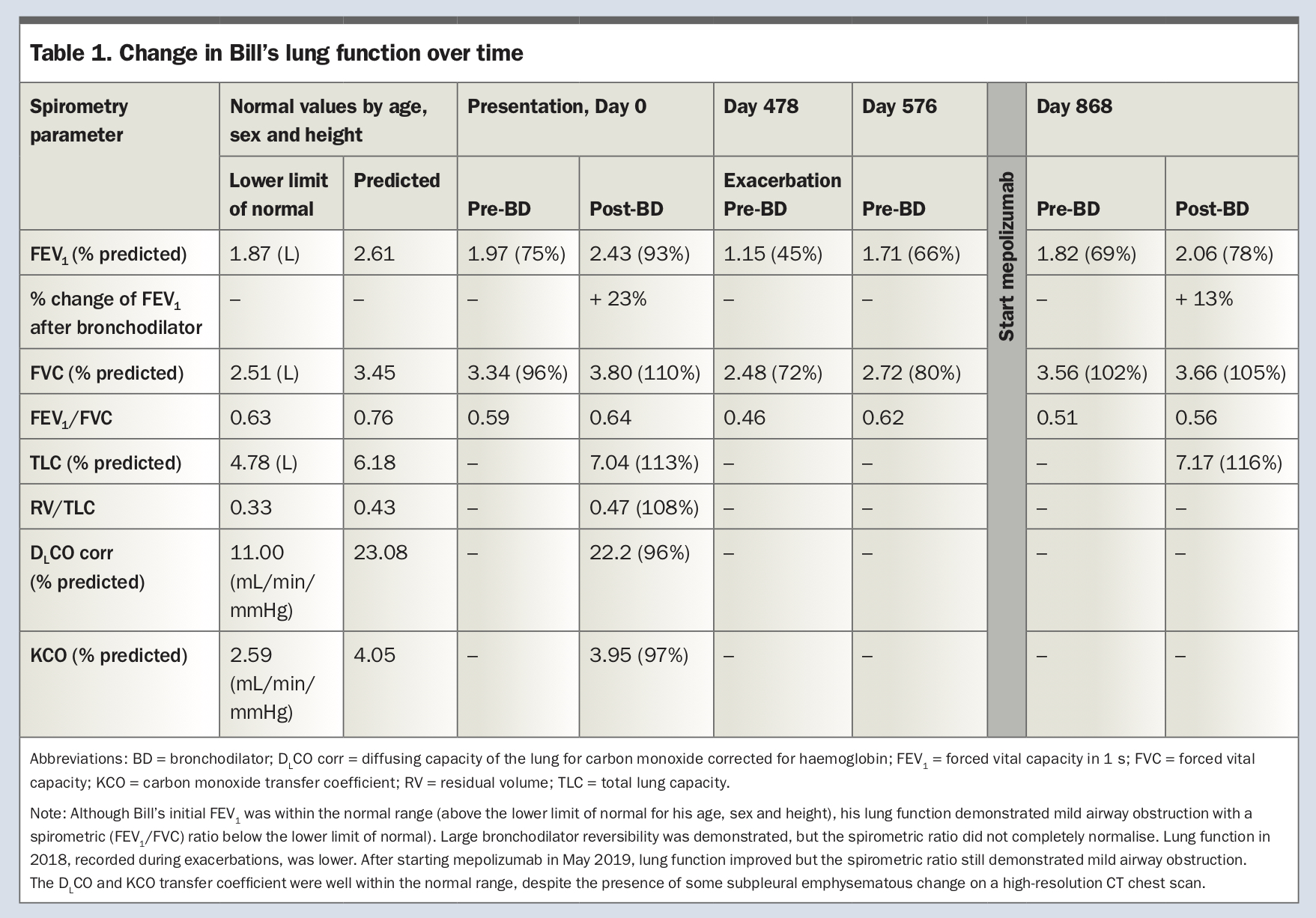
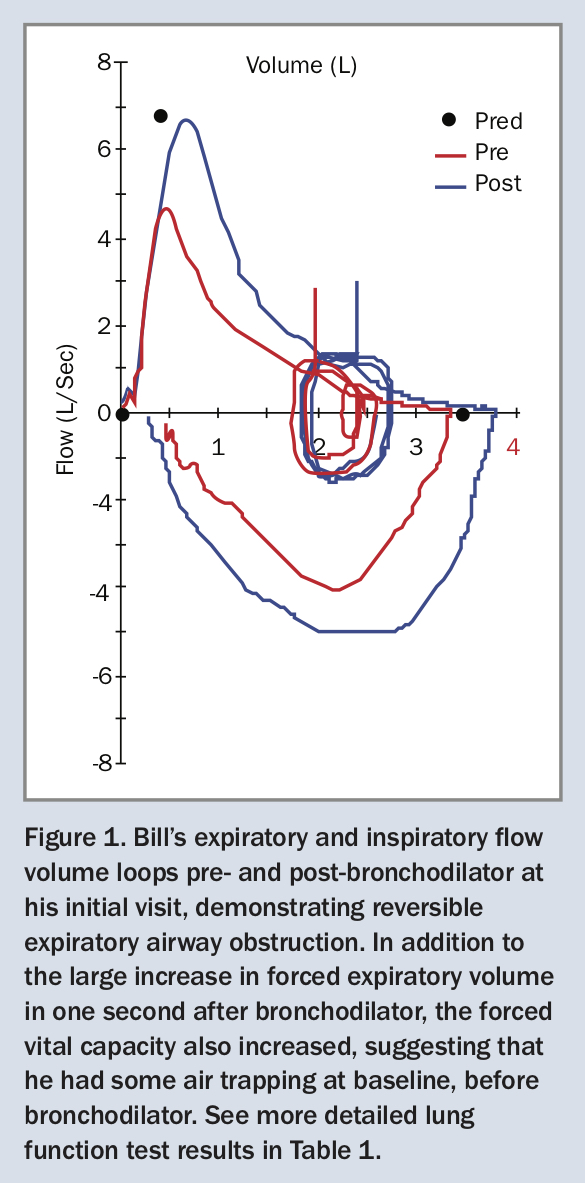
At this time, his spirometry shows moderate airflow limitation with substantial bronchodilator reversibility (now called ‘bronchodilator responsiveness’; Table 1 and Figure 1) and the following results:
{kind=link}
{kind=link}
- forced expiratory volume in one second (FEV1) before salbutamol administration, 1.97 L (75% predicted)
- FEV1 after two puffs of salbutamol, 2.43 L (93% predicted)
- forced vital capacity (FVC) before salbutamol administration, 3.34 L (96% predicted)
- FVC after salbutamol administration, 3.80 L (110% predicted)
- FEV1/FVC 0.59; after four puffs of salbutamol, FEV1/FVC was 0.64
- diffusing capacity of the lung for carbon monoxide, corrected for haemoglobin (DLCO corr) 22.2 mL/min/mmHg (96% predicted).
The diagnosis of asthma is confirmed by the very large bronchodilator responsiveness in FEV1 of +23% and +460 mL from baseline. According to American Thoracic Society/European Respiratory Society criteria, significant responsiveness is considered to have been demonstrated if there has been a 12% and 200 mL (or greater) improvement in FEV1 and/or FVC from baseline.1 Patients with chronic obstructive pulmonary disease (COPD) can have some bronchodilator responsiveness but the greater the change after bronchodilator, the more likely the diagnosis of asthma (Figure 1).
Bill is initially given a written asthma action plan, and the dose of his ICS/ LABA (fluticasone propionate/salmeterol 250 mcg/25 mcg) is increased to two puffs twice daily with a spacer. Salbutamol via pressure metered-dose inhaler is also prescribed, to be taken two puffs with a spacer, as needed. He is taught correct inhaler technique and this is reviewed again on subsequent visits. Bill notes some improvement with these interventions, but his respiratory symptoms still occur frequently. Next, a long-acting muscarinic antagonist (LAMA) – tiotropium 2.5 mcg two inhalations daily via misthaler device – is added, providing some additional relief. Bill is referred to cardiopulmonary rehabilitation after appropriate cardiac investigations excluded cardiac ischaemia. He also reports symptoms of chronic GORD, despite a previous fundoplication for it, and continues with regular proton pump inhibitor therapy. Given Bill’s underlying anxiety, which may be contributing to episodes of dyspnoea, he is referred to a psychologist for ongoing support and dyspnoea management.
Over the next 12 months, Bill is seen regularly at a specialist respiratory clinic and reports excellent adherence to his ICS/LABA and LAMA. Despite this, Bill is admitted to hospital on five occasions over the 12 months, with severe exacerbations of asthma requiring systemic corticosteroids. One of these exacerbations requires intensive care unit (ICU) admission and intubation. In addition to maximal dose ICS/LABA + LAMA, Bill is started on oral prednisolone, initially 50 mg daily during an exacerbation. However, he is subsequently unable to be weaned to below 20 mg throughout the year.
As part of his work-up for possible biologic add-on therapy, Bill also has the following investigations:
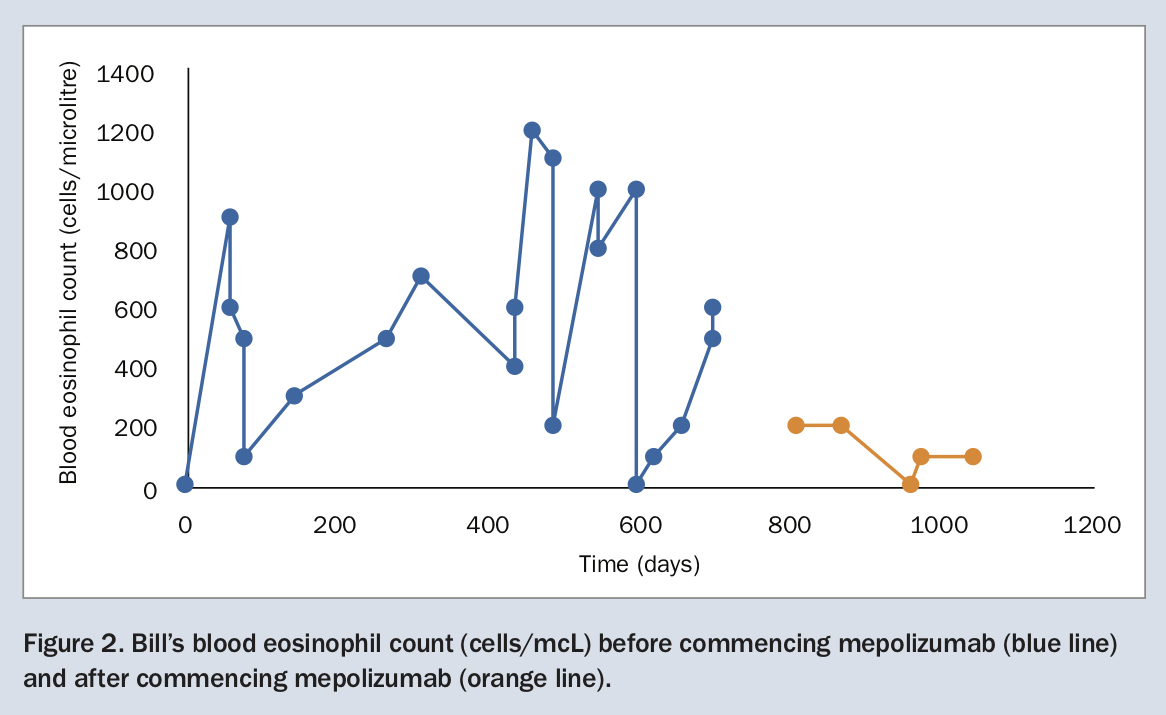
- blood eosinophil count: ranging between 400 and 1200 cells/mcL over 12 months
- immunoglobulin (Ig) E antibodies: 42 kU/L (upper limit of normal [ULN] 120 kU/L)
- skin prick testing negative to common aeroallergens
- Aspergillus fumigatus IgG antibodies: negative
- CT chest scan: demonstrating mild bilateral apical scarring and subpleural emphysematous change, both at the apices and adjacent to the pericardium.
Does Bill qualify for biologic therapy? Which monoclonal antibody therapy is most likely to help him?
Commentary
In summary, Bill has severe adult-onset eosinophilic asthma, with frequent severe exacerbations requiring hospitalisation despite high-dose ICS/LABA and regular LAMA as add-on therapy. His symptoms appear to be due mainly to asthma, rather than being attributable to comorbidities such as GORD or anxiety. The main differential diagnosis here is COPD given Bill’s smoking history and subpleural emphysematous change seen on CT. It seems likely that Bill does have a component of COPD; however, the significant bronchodilator response (23% and 460 mL), normalisation of spirometry after bronchodilator and elevated eosinophil count indicate a predominant asthma phenotype. Despite good adherence to inhaled therapy and correct inhaler technique, he continues to have exacerbations. He is now dependent on systemic corticosteroids and his respiratory symptoms continue to greatly limit his activities of daily living. Therefore, he should be considered for biologic therapy. Given the high levels of blood eosinophils and frequent exacerbations, including while on maintenance prednisolone, anti-eosinophil therapy would be the biologic of choice.
There are several factors in Bill’s case that suggest he has a severe asthma phenotype that is likely to benefit from targeted biologic therapy.
First, Bill has adult-onset asthma with intermittent wheeze and dyspnoea, and severe and frequent exacerbations requiring ICU admission and intubation. These have occurred despite good adherence to optimised inhaler therapy (high-dose ICS/LABA) including the addition of a LAMA and correct technique. The persistence of symptoms and/or exacerbations despite optimised high-dose standard therapy and management of contributory conditions satisfies the current definition of severe asthma; that is, asthma that is relatively refractory to conventional treatment.2,3
Bill is now dependent on high-dose systemic corticosteroids, both to treat his severe exacerbations as well as to reduce his daily symptoms of persistent wheeze and breathlessness. This suggests a strong component of airway inflammation that is driving his uncontrolled symptoms. Use of maintenance oral corticosteroid (OCS) is associated with a greatly increased risk of adverse events such as diabetes, osteoporosis, obesity and depression, so it is a priority to be able to reduce or cease OCS.4 Anti-eosinophil biologics are very effective at reducing the need for OCS.5,6
In addition, Bill’s persistently raised blood eosinophil count despite high-dose ICS and even OCS suggests that his symptoms are driven by eosinophilic airway inflammation, a process that, in patients with severe asthma, can be targeted by new biologic agents such as mepolizumab or, more recently, benralizumab (Table 2). On multiple occasions in the preceding 12 months, Bill’s blood eosinophil levels have been greater than 1000 cells/mcL, significantly above the ULN of 500 cells/mcL. Bill does not have any known allergies and he only identifies chocolate and perfumes as potential triggers for his symptoms. He is nonatopic as indicated by negative reactions to a standard panel of aeroallergens on skin prick testing. If the clinical history had suggested any allergens as potential triggers, his atopic status could also have been documented with specific IgE testing for relevant allergens. Although classically thought to be associated with severe atopic asthma, high eosinophil counts are also seen in patients with nonatopic severe asthma.7,8
{kind=link}
Patients with adult-onset asthma – compared with those with childhood-onset asthma – are more likely to have nonallergic asthma and more severe airflow limitation, although allergic asthma is also seen, including in occupational asthma.9 Severe eosinophilic asthma is often associated with nasal polyposis, but Bill’s good sense of smell and nonobstructed nose make it unlikely that he has nasal polyps.
Diagnosis of severe asthma
Severe asthma comprises less than 4% of all asthma, and is defined as asthma that remains uncontrolled despite regular treatment with high-dose ICS plus LABA or with maintenance OCS, or asthma that requires this level of treatment to prevent loss of control.10,11 Importantly, asthma severity is defined by the level of treatment required to control symptoms and exacerbations, rather than by the intensity of frequency of symptoms or other clinical parameters.
In the diagnosis of severe asthma, it is important to first establish that the underlying asthma diagnosis itself is correct. As patients often have longstanding asthma, and may have developed persistent airway obstruction, the diagnosis usually needs to be confirmed by a specialist experienced in the care of patients with severe asthma. It is very important to assess adherence to conventional therapy including inhaler technique, and to identify and treat any coexisting conditions. In many cases, addressing these critical steps is enough to downgrade a classification of severe asthma.12,13
There are numerous differential diagnoses or comorbidities that may contribute to respiratory symptoms including current smoking, COPD, allergic rhinitis, GORD, obstructive sleep apnoea, obesity, mental health disorders, upper airway dysfunction and allergic bronchopulmonary aspergillosis. Referral to a specialty asthma clinic increases the identification of coexisting conditions, and, in many cases, effectively treating comorbidities can improve outcomes and avoid the need for costly biologic therapy.14,15 Of note, Bill has a significant smoking history, late adult onset of respiratory symptoms, and presence of emphysema on his CT scan, suggesting mixed features of asthma and COPD, or asthma-COPD overlap.16 His GORD, obesity and anxiety also need to be addressed in his overall management.
Management
An integrated multidisciplinary approach
Before considering biologic therapy for severe asthma, all patients should ideally undergo assessment and optimisation of treatment at a specialist respiratory clinic that is experienced in the management of severe asthma, as described above. A multidisciplinary clinic may include a clinical nurse educator, pharmacist, physiotherapist and psychologist in addition to physicians who can prescribe biologic therapy (respiratory physicians, allergists, immunologists or general physicians, expert in managing severe asthma). However, initial assessment and management of modifiable risk factors can also be carried out in primary care. The GINA (Global Initiative for Asthma) pocket guide to severe asthma and a toolkit produced by the Australian Centre of Excellence in Severe Asthma, both of which are available online, provide excellent practical resources for diagnosis and management of severe asthma.2,17
Fundamental management of severe asthma includes confirming the diagnosis, providing a written asthma action plan, checking inhaler technique and continuing to encourage adherence. A trial of low-dose budesonide/formoterol (eformeterol) as single maintenance-and-reliever therapy (MART) with, for difficult-to-treat asthma, a medium maintenance dose (e.g. budesonide/ formoterol (eformeterol) 200/6 turbuhaler two inhalations twice daily and one inhalation as needed for symptom relief) may be beneficial, particularly if adherence to regular ICS/LABA is in question.18 A trial of add-on tiotropium (via mist inhaler) may increase lung function and time to first exacerbation.19,20 Tiotropium is only subsidised by the PBS when used in combination with high-dose ICS/LABA for people with one or more previously documented severe exacerbations that required systemic corticosteroids in the previous 12 months (www.pbs.gov.au). The annual influenza vaccine and five-yearly pneumococcal vaccine are also recommended.2 For patients with anxiety, it may be helpful for the general practitioner to include this as part of a chronic care plan, to allow access to subsidised psychology services.
Biologics
What monoclonal antibodies are available in Australia to manage severe asthma?
Biologic therapy in severe asthma comprises humanised monoclonal antibodies that disrupt the type 2 inflammatory pathway. Type 2 inflammation, which is named after T helper 2 (Th2) cells, is found in about 50% of people with asthma, across the spectrum of severity. It is characterised by cytokines such as IL-4, IL-5 and IL-13, which are often produced by the adaptive immune system when it recognises allergens and parasites. Type 2 inflammation may also be activated by viruses, bacteria and irritants that stimulate the innate immune system via production of IL-33, IL-25 and thymic stromal lymphopoietin (TSLP) by epithelial cells. Type 2 inflammation is often characterised by elevated blood and/or sputum eosinophils. In many patients with asthma, type 2 inflammation rapidly improves with ICS treatment (provided it is taken correctly). However, in severe asthma, type 2 inflammation may be relatively refractory to high-dose ICS. Although it may respond to OCS, these have serious side effects, so the introduction of biologic therapy has provided an important additional therapeutic approach for patients with severe asthma.
In Australia, there are currently three biologics subsidised by the PBS for severe asthma and, due to their high cost, each has strict PBS prescribing criteria (Table 2). Specific eligibility criteria for each biologic and up-to-date product information are available on the PBS website (www.pbs.gov.au) and TGA website (www.tga.gov.au), respectively, and practical advice about choice and administration of monoclonal antibodies is included in the Australian severe asthma toolkit.21
Mepolizumab and benralizumab are humanised monoclonal antibodies that target IL-5 and the IL-5 receptor alpha subunit, respectively. Both these agents are considered anti-eosinophil therapies, as IL-5 is the main cytokine involved in the proliferation and differentiation of eosinophils.21 In the case of benralizumab, binding the IL-5 receptor directly induces eosinophil apoptosis.21
Omalizumab is a humanised monoclonal anti-IgE antibody, which binds to the Fc (fragment crystallisable) portion of free IgE to prevent free IgE binding to IgE receptors.21 IgE plays a critical role in the allergic cascade, particularly when bound to IgE receptors on the surface of mast cells and basophils. In the presence of a specific allergen, crosslinked IgE triggers a cascade of changes including the release of vasoactive inflammatory mediators, proinflammatory cytokines and other chemoattractant mediators from mast cells and basophils, and thus induces the airway oedema and smooth muscle contraction that lead to asthma symptoms such as bronchoconstriction and mucus production.
Which monoclonal antibody is most likely to benefit my patient?
It is helpful to characterise each patient’s severe asthma phenotype, in order to choose the appropriate biologic agent. As in Bill’s case, confirmation of the severe asthma phenotype is guided by biomarkers including blood eosinophil count, serum IgE and, if available, exhaled fraction of nitric oxide (FeNO).
Therapies targeting IL-5/IL-5 receptor (mepolizumab and benralizumab) are most beneficial in patients with uncontrolled severe eosinophilic asthma, who have had two or more exacerbations in the past year and have an eosinophil count greater than or equal to 300 cells/mcL.22,23 As OCS may (partly or completely) suppress the blood eosinophil count, PBS criteria now also permit treatment with these drugs for a blood eosinophil count greater than or equal to 150 cells/mcL while the patient is receiving treatment with OCS.24 Bill meets these criteria and would be eligible for anti-IL-5 therapy. In patients with severe eosinophilic asthma, both have been shown to reduce asthma exacerbations and asthma symptoms.5,6,25,26 Both drugs have been shown to decrease oral corticosteroid dose by about 50%.5,6 The effect on FEV1 is only small to moderate.26,27
Omalizumab, which binds free IgE, is indicated as add-on therapy in patients with severe allergic asthma, with IgE level equal to or greater than 30 IU/mL, and a positive skin prick test or elevated specific IgE level in response to an aeroallergen (examples are house dust mite and cat).24 In these patients, anti-IgE therapy has been shown to decrease frequency of exacerbations and slightly reduce symptoms, with minimal effect on FEV1.28,29
What are the current PBS criteria for initiation of biologics in Australia?
In brief, from December 2019, the general PBS criteria for all the biologic therapies include treatment by a respiratory physician, clinical immunologist, allergist or general physician experienced in the management of patients with severe asthma attached to an approved hospital, for patients under their care for at least six months; or treatment by a multidisciplinary severe asthma team. The patient must have had asthma for at least one year, with confirmation of the diagnosis by a specialist, with demonstration of significant bronchodilator responsiveness or airway hyperresponsiveness. However, if these tests are not positive for asthma (as is often the case for patients with longstanding asthma), the diagnosis can be confirmed by two specialists expert in the management of severe asthma. Finally, the patient must have inadequate asthma control despite documented adherence to optimised standard treatment including high-dose ICS/LABA for at least 12 months, and evidence of OCS use for severe exacerbations. For severe eosinophilic asthma and severe allergic asthma, specific biomarkers are also required to determine eligibility for the relevant biologic therapy.
All three of these biologics are PBS-subsidised for patients 12 years and older. Omalizumab is also PBS-subsidised for severe allergic asthma in children aged from 6 years to below 12 years. Criteria for all three biologics are available on the Services Australia website.30 See Box for practice points.
Can my patient switch to a different biologic agent?
A number of patients with severe asthma may meet PBS criteria for more than one monoclonal antibody agent. Until recently, the PBS required patients with adverse reactions or incomplete response to complete a six-month washout period between different biologics. Recently, the PBS has made it easier to switch between monoclonal antibody therapies.31 The gap between therapies is now only one month. The treating physician now has greater flexibility to tailor the choice of biologic agent or agents to their patient’s requirements, so long as the patient qualifies for the agent. Criteria for ongoing therapy include reduced symptoms and/or reduced maintenance OCS; details are available on the Services Australia website.32
Bill’s progress
After 12 months of poor asthma control despite optimal high-dose ICS/LABA, systemic corticosteroids and tiotropium therapy, Bill is started on mepolizumab subcutaneous injection once per month, in addition to his previous medications. Over the next six months, Bill feels that his daily asthma symptoms improve somewhat in the first two weeks after each mepolizumab infusion, but he returns to persistent daily wheeze in the one to two weeks before the next infusion is due. He continues to have significant exercise limitation to less than 50 m before rest. However, while being treated with mepolizumab, Bill is only hospitalised once with an asthma exacerbation, which was triggered by a respiratory viral infection. He is also weaned off systemic corticosteroids down to 5 mg prednisolone daily, when compared with a minimum of 20 mg daily before biologic therapy. His blood eosinophils are eventually suppressed to below 100 cells/mcL (Figure 2). This represents an encouraging but clinically incomplete response to biologic therapy. Bill’s other comorbidities such as anxiety, obesity and GORD may also be contributing to his ongoing symptoms, particularly dyspnoea. For patients with no response, or partial response (such as Bill), to initial biologic therapy, recent changes in the PBS criteria for switching between monoclonal antibody therapies mean that they will now also have more timely access to an alternative biologic agent that may provide greater benefit. RMT
{kind=link}
COVID-19 and asthma
Advice from the authors of this article on managing patients with asthma during the COVID-19 pandemic is provided in the Box.