Improving adherence to treatment in COPD. A personalised approach


COPD (chronic obstructive pulmonary disease)
Breathing problems
Nonadherence is a multidimensional quandary in patients with chronic obstructive pulmonary disease and encompasses a range of physical, economic, psychological and social factors. When assessing for nonadherence, engaging with patients to understand these factors is essential to formulating tailored, long-term strategies and interventions.
- Nonadherence to chronic obstructive pulmonary disease (COPD) medications is common and is associated with poor clinical outcomes.
- Nonadherence can result from patient, treatment, health professional or health system factors.
- It can be classified into intentional and unintentional nonadherence.
- Each form of nonadherence requires a personalised solution.
- Structured questionnaires, smart inhalers and patient-centred communication are useful in promoting adherence.
Nonadherence continues to be a major source of frustration for health professionals as it not only contributes to morbidity and mortality, but also results in economic costs and waste of resources. The WHO has recognised the importance of enhancing adherence as a strategy to tackle chronic conditions effectively.1 This article focuses on how GPs can engage with patients to help improve adherence to treatment in chronic obstructive pulmonary disease (COPD).
Adherence
Adherence is defined as ‘the extent to which a person’s behaviour (in terms of taking medications, following diets or executing lifestyle changes) coincides with medical or health advice’ and is a key determinant of health outcomes.1 Definitions for adherence often refer to the amount of medicine taken or treatment received over a given period, or the extent to which medication use correlates to factors such as recommended timing, intended duration and recommended method of use. Adherence to medically prescribed treatment and/or preventive measures ranges from 4.6 to 100% (average, 75.2%) and is dependent on:2
- method of assessment
- focus characteristic chosen for assessment (e.g. use of regular oral medications, inhaler technique)
- operational definitions (e.g. defining 80 to 120% utilisation of regular medications as good adherence)
- patient population
- time points of assessments
- practice setting
- assessor background.
Nonadherence
Given the range of reported adherence for various settings we should now examine nonadherence. This term is commonly used in clinical practice and scientific literature as shorthand for ‘partial adherence’, ‘suboptimal adherence’ or ‘poor adherence’.3 Nonadherence can be further defined as ‘primary nonadherence’, when the patient fails to initiate the treatment (e.g. no medicine dispensed, rehabilitation not started), and ‘secondary nonadherence’, when the treatment is not followed as intended (e.g. doses missed, rehabilitation program discontinued early).
Nonadherent behaviour can be broadly classified as ‘unintentional nonadherence’ and ‘intentional nonadherence’. Unintentional nonadherence can result from simple forgetfulness (defined by the WHO as ‘erratic nonadherence’) or inability to follow treatment instructions (e.g. incorrect inhaler technique) because of a lack of understanding or physical problems such as poor eyesight or dexterity (defined by the WHO as ‘unwitting nonadherence’). Intentional nonadherence (also called ‘intelligent nonadherence’) arises when the patient rejects either the doctor’s diagnosis or the doctor’s recommended treatment, based on a ‘rational decision’.1,3 It is likely that these adherence ‘phenotypes’ could occur alongside each other within the same patient.
Nonadherence in patients with COPD
In a symptomatic condition such as COPD, it is logical to think that patients would be highly adherent to their treatment. However, poor adherence to treatment and disease management programs has been identified as the major factor resulting in emergency hospitalisation in those with COPD.4 Nonadherence is a multi-dimensional quandary in COPD, with both intentional and unintentional nonadherence being common, and includes:
- short- and long-term medication nonadherence
- nonadherence to lifestyle changes such as smoking cessation
- nonparticipation in or early withdrawal from respiratory rehabilitation or exercise programs
- failure to meet vaccination requirements
- missing scheduled clinic or home visits
- inadequate monitoring of treatment response.
Generally, adherence to health-enhancing lifestyle behaviours has been found to be even worse than adherence to medications.3 Three patterns of nonadherence are common in patients with COPD: ‘underuse’, ‘overuse’ and ‘inappropriate use’, especially poor inhaler technique.
Nonadherence is a multifaceted issue influenced by a range of patient-, medication-, healthcare provider- and health system-related factors.5 Common risk factors for medication nonadherence include polypharmacy (use of two or more medications for at least 60 days per quarter per year), especially inhaler device polypharmacy, cognitive and functional decline, inadequate health professional contact, depressive symptoms, poor social support and absence of assistance with medication administration. Reasons given by patients with COPD for poor adherence to their treatments include:6
- forgetfulness
- deciding not to take a dose because of interruptions or changes in routine
- not taking a dose because of side effects or fear of side effects
- running out of medications
- physical difficulty or inconvenience
- lack of time
- social stigma
- feeling of lack of need for treatment
- lack of effect or perceived benefit from treatment
- absence of symptoms.
Strategies for addressing adherence issues in patients with COPD
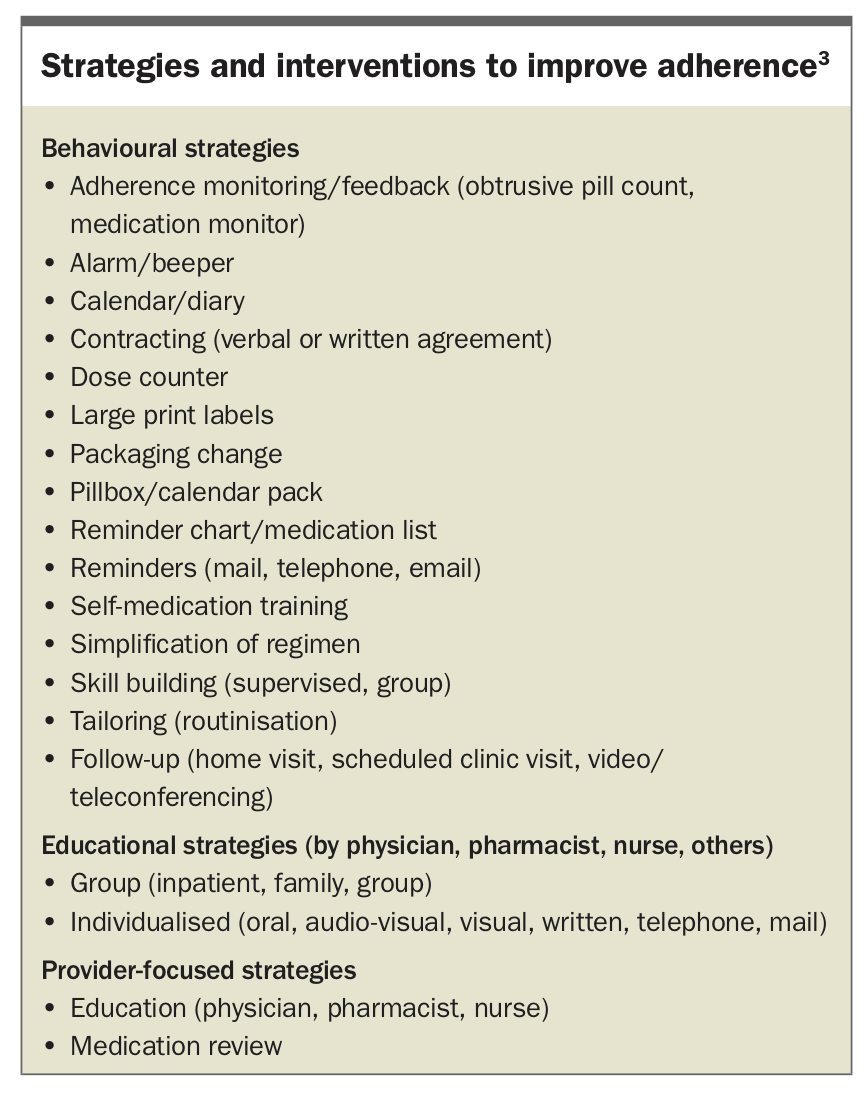
Adherence is a multifactorial issue in COPD and can be best understood in the context of patients’ physical, economic, psychological and social circumstances. Awareness of the factors pertaining to nonadherence from the patient’s perspective is essential to formulating tailored long-term strategies to address those issues. A variety of strategies for improving adherence can be used individually or in combination (Box).3
{kind=link}
Due to lack of information about a patient’s nonadherence, practitioners often try to address both unintentional and intentional nonadherence using the same intervention. Educational and motivational strategies are likely to be required to address intentional nonadherence, whereas behavioural and provider-focused strategies, such as medication review focused on regimen simplification, are more likely to be successful in addressing unintentional nonadherence.
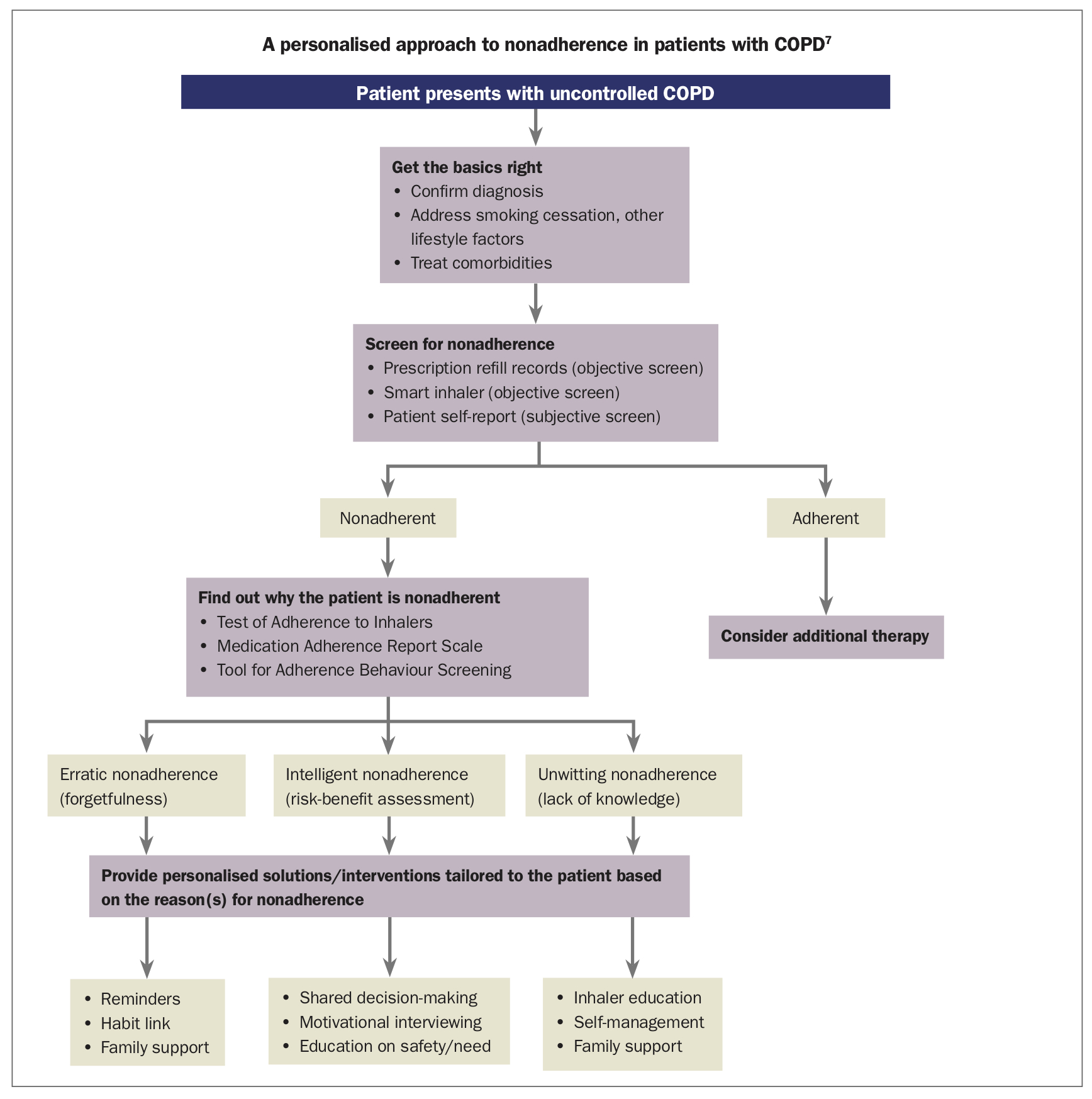
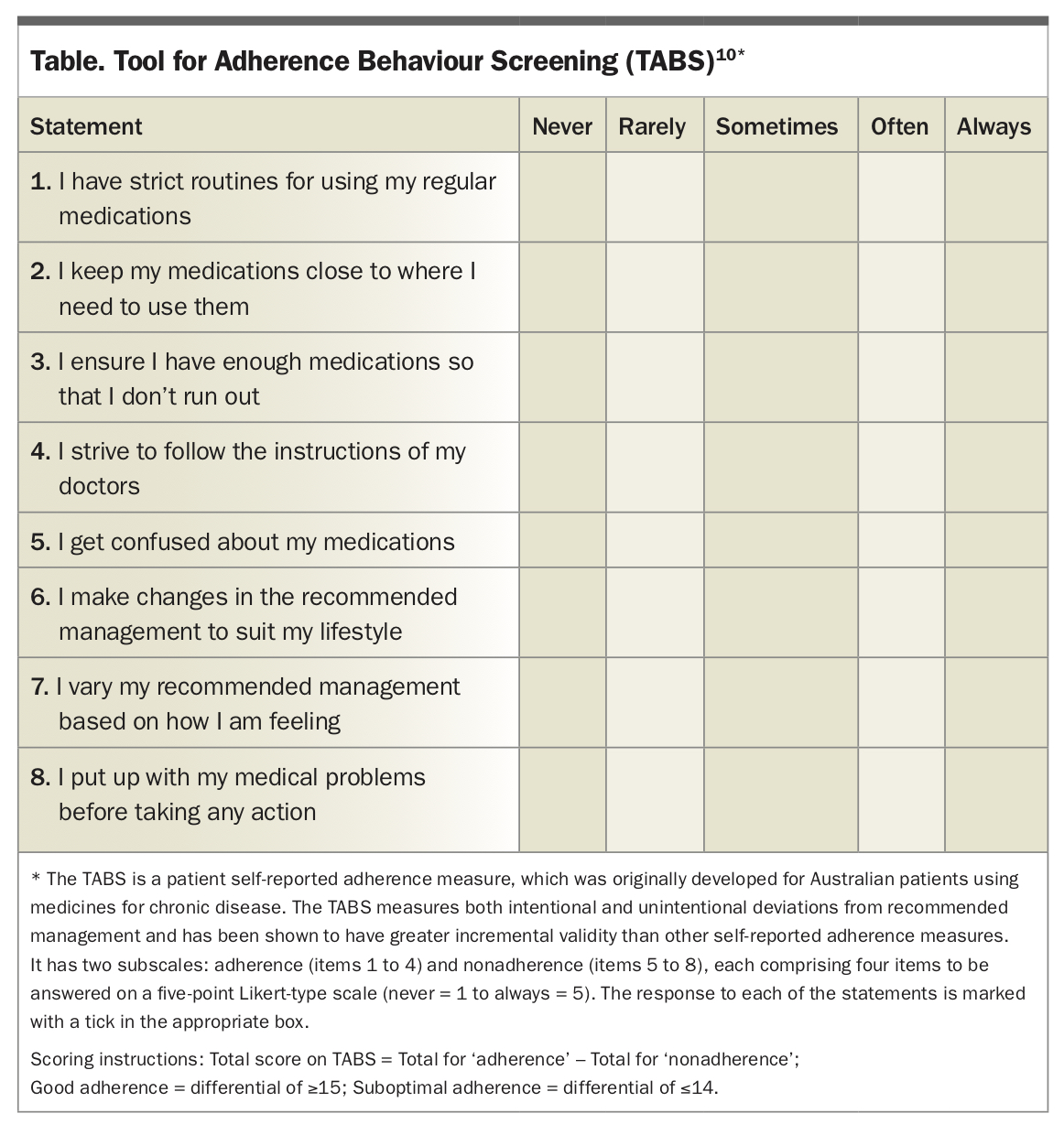
A stepwise approach can be used for improving adherence (Flowchart).7 First, when uncontrolled COPD is signalled, the clinician should check that the basics are right; that is, ensure diagnosis is correct, lifestyle factors have been addressed and comorbidities treated (see the Lung Foundation Australia’s COPD-X Concise Guide8). Then, nonadherence should be assessed. Detection of nonadherence (e.g. from prescribing or dispensing data or, in the future, smart inhalers) and characterisation of the nature of nonadherence using simple questionnaires or open-ended questions are essential before selecting specific intervention strategies. There exist short and well-validated generic questionnaires such as the Medication Adherence Report Scale, Tool for Adherence Behaviour Screening (Table) and the Test of Adherence to Inhalers.9-11 They provide quantitative and qualitative insights into the extent of and underlying reasons for nonadherence.
{kind=link}
{kind=link}
If nonadherence is suspected, one or more tailored solutions should be offered. These often involve a medication review to assess the appropriateness of the patient’s medications, their ability to use the inhaler and simplification of the regimen if possible (e.g. combination inhaler) or use of identical inhalers or those with very similar mechanisms. GPs may want to consider referral to a consultant pharmacist for a Home Medicines Review (MBS rebate available) to assist with assessment and implementation of strategies to address nonadherence. Importantly, all healthcare professionals involved in inhaler technique training should keep their own inhaler teaching skills up to date.
If erratic nonadherence (forgetfulness) is the primary cause of nonadherence, telephone reminders could be set and dosing times tailored to fit in with the patient’s daily routine (routinisation) or linked to daily activities (e.g. brushing teeth) and, if possible, family members or caretakers involved. In cases of intelligent nonadherence, patient interviews focusing on the importance of adherence and the potential consequences of nonadherence should be offered; this must be handled in a nonaccusatory manner to maintain rapport.
In cases of polypharmacy, a multicompartment dose administration aid may be recommended, if appropriate. Those with peripheral sensory problems or visual impairments may have difficulty removing capsules from packs or bottles to put into a device, or using devices that require careful observation for dose preparation or delivery. Any adherence aid (e.g. aids for easy actuation of puffers by those with rheumatological or musculoskeletal difficulties) should be chosen in consultation with the patient and should match the patient’s abilities as different aids require varying manipulative skills. Phone or text reminders for clinic appointments and prescription refills are common. Mobile health and home monitoring devices with capabilities for real-time monitoring of symptoms and data through bluetooth-enabled gadgets attached to inhalers (‘smart inhalers’) and feedback on disease management, including treatment adherence are also becoming widely available.12
Regardless of the number and types of interventions, some patients will remain nonadherent in the longer term. They need to be supported and not blamed. Retraining patients in the primary care setting, especially after recovery from exacerbations and hospitalisations, will be highly beneficial. Health professionals should show empathy towards such patients and keep supporting them with periodic review of their adherence and suitable adherence enhancement measures.
Conclusion
Adherence to treatment continues to be a major challenge in patients with COPD. A true partnership among doctors, pharmacists and patients is critical for optimising adherence, and will result in better health outcomes. RMT