ONLINE FIRST: Silent hypoxaemia in COVID-19. What does it mean?


A unique presentation of silent hypoxaemia – minimal dyspnoea associated with profound hypoxaemia – has been reported in patients with COVID-19. The management of silent hypoxaemia requires early recognition, as these patients are at risk of rapid deterioration and respiratory failure. Early recognition of this phenomenon can be challenging for patients who are being monitored in the community. However, pulse oximeters are a simple tool that can be useful for identifying patients with silent hypoxaemia in the community and in hospital.
- Silent hypoxaemia is an apparently unique phenomenon in patients with COVID-19 where profound hypoxaemia is demonstrated without dyspnoea or clinical symptoms of respiratory distress.
- Patients with silent hypoxaemia are at risk of rapid deterioration and respiratory failure. Therefore, early detection is important.
- Pulse oximetry can be used to estimate arterial oxygen saturation and allow for remote monitoring of patients with COVID-19 in the community when hospitalisation is not required, enabling follow up by healthcare providers (e.g. phone or telehealth consultations). Many outpatient programs are providing patients with equipment for self- monitoring in the home setting.
- The underlying mechanisms of silent hypoxaemia are not understood and little is known about long-term sequelae.
The coronavirus disease 2019 (COVID-19) outbreak has led to a global pandemic affecting tens of millions of people and causing millions of deaths worldwide. In Australia, over 45,000 confirmed cases have occurred at the time of writing, and numbers continue to increase.1
COVID-19 is caused by infection with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).2 Patients with COVID-19 typically present with symptoms and signs related to respiratory tract infection.3 Fever, cough, dyspnoea and myalgia are common presenting symptoms; however, clinical manifestations related to other organ systems, including the gastrointestinal tract and cardiac, neurological and vascular systems, have also been reported.4,5 The spectrum of COVID-19 severity is variable – the range includes patients who are asymptomatic, those with mild and self-limiting upper respiratory tract symptoms, and patients who have severe disease with acute respiratory distress syndrome (ARDS) and/or respiratory failure and death.4,6
An unique presentation that has been widely reported in patients with COVID-19 is that of no or minimal dyspnoea associated with profound hypoxaemia.7-10 This phenomenon has been coined ‘happy hypoxaemia’ or ‘happy hypoxia’, which is somewhat misrepresentative because patients with COVID-19 are not happy but potentially very unwell.11 A more fitting description – ‘silent hypoxaemia’ or ‘silent hypoxia’ – has also been used.12
What is silent hypoxaemia?
Silent hypoxaemia is characterised by significant hypoxaemia without the expected features of respiratory distress.9,10,12,13 The patient is alert and conscious but lacks awareness of the hypoxaemia and reports no dyspnoea. Concurrent computed tomography imaging of the lungs may demonstrate consolidation and/or ground glass opacification.14 An example is described in the Box.
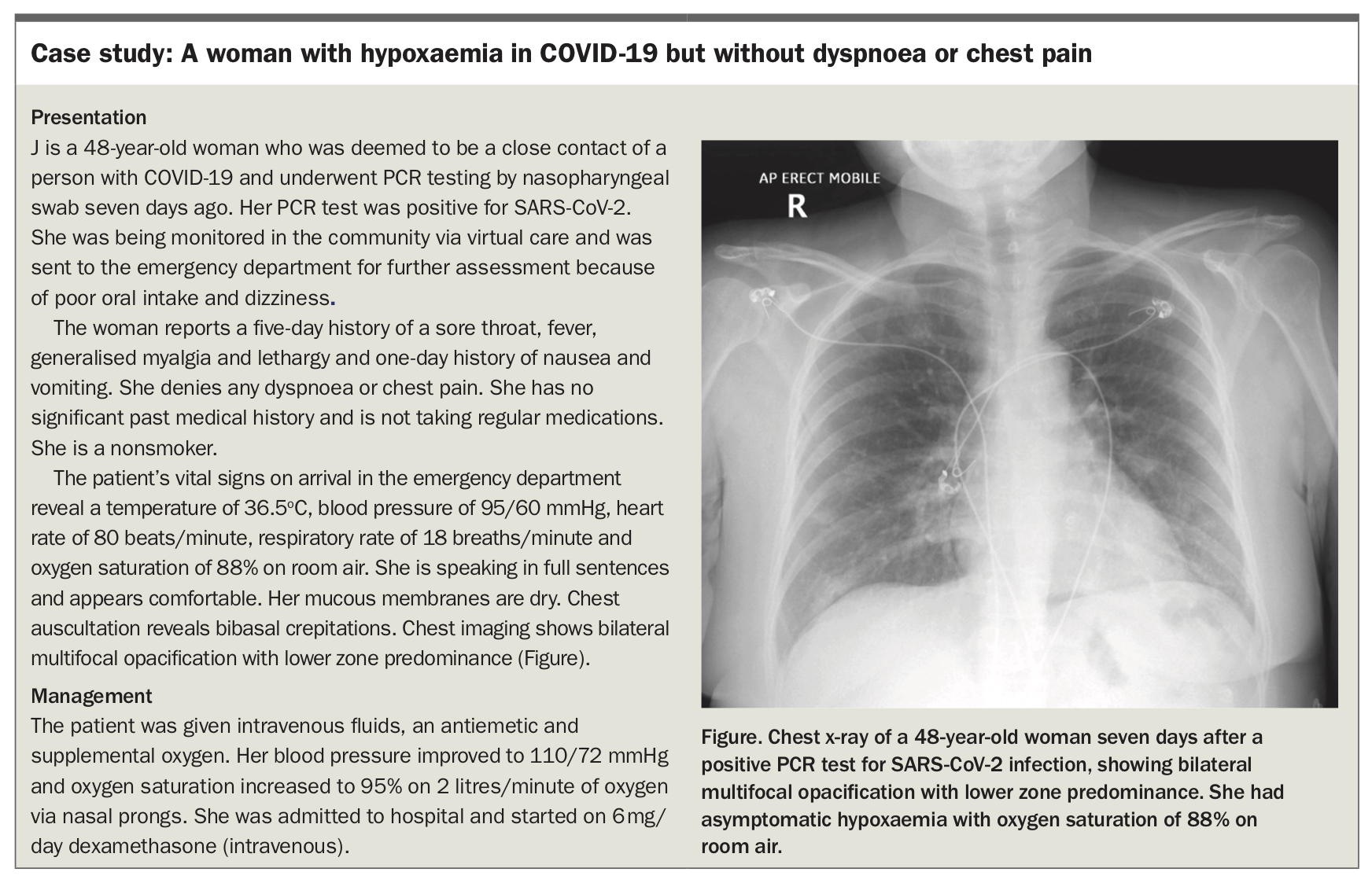{kind=link}
Although there is no standardised definition for silent hypoxaemia, oxygen saturation measured by pulse oximetry (Sp02) and arterial oxygen pressure levels as low as 70% and 40 mm Hg, respectively, have been reported in asymptomatic patients with COVID-19.15 There are limited data on the severity of hypoxaemia in asymptomatic patients with COVID-19 and the prevalence of silent hypoxaemia is not known. Reports suggest the prevalence to be between 20 and 40%; however, this may not be a true reflection because concurrent oxygen saturation measurements and dyspnoea scores were not recorded.8 Moreover, some reports may have included patients without dyspnoea who had not yet developed hypoxaemia.7
Silent hypoxaemia poses a major risk to patients because the subjective sensation of dyspnoea and clinical signs of respiratory distress are not present. It may be associated with an increased risk of mortality and poor outcomes.16-18 Furthermore, up to one-third of patients with COVID-19 lung injury and without dyspnoea or signs of respiratory distress can rapidly develop severe disease with respiratory failure and subsequent ARDS.4
Diagnosis of silent hypoxaemia
Subjective dyspnoea measurements and self-reported symptoms of shortness of breath have been used to risk stratify patients with COVID-19. However, these are insufficient to accurately detect hypoxaemia in patients who are considered high risk for severe COVID-19; thus, objective tools are required.19
Pulse oximeters, a simple and noninvasive tool, can be used to estimate arterial oxygen saturation. These tools, which are cheap and easy to use, are typically available as a device that is placed over a finger. They allow for remote monitoring of patients with COVID-19 in the community when hospitalisation is not required.19,20,21 Further information is available from the RACGP website (see https://www.racgp.org.au/clinical-resources/covid-19-resources/other-health-issues/home-care-guidelines-patients-with-mild-covid-19 and https://www.racgp.org.au/download/Documents/Standards/RACGP-Standards-for-general-practices-5th-edition.pdf).
It is crucial to recognise factors that may result in measurement error and affect pulse oximeter accuracy. Factors to consider include rapid measurement fluctuation when the arterial oxygen pressure/tension falls on the steep portion of the oxygen dissociation curve and diminished pulsatile blood flow due to hypotension, vasoconstricting medications or peripheral vascular disease.20 The increased skin pigmentation of some individuals and the use of nail polish can also affect readings.20 Additionally, the accuracy may vary depending on the type of pulse oximeter device, particularly when oxygen saturation falls below 90%.20 Issues arising from incorrect placement of the pulse oximeter over a finger can be overcome by instead using an earlobe or forehead probe; however, these devices are not readily available and are more costly than finger pulse oximeters.
Arterial blood gas (ABG) analysis is a more invasive tool that can be used to accurately detect hypoxaemia. This involves measurements of the pH and partial pressures of oxygen and carbon dioxide in arterial blood and provides information about a patient’s acid-base balance, the effectiveness of gas exchange and state of their ventilatory control. An ABG analysis requires a blood sample, usually drawn from the radial artery, and is generally not feasible to perform in the community.
How and why do patients present with silent hypoxaemia?
Hypoxaemia is often associated with dyspnoea, but the mechanisms underpinning the sensation of dyspnoea are complex and not completely understood. Factors that can contribute to dyspnoea include changes to the respiratory muscles, CO2 receptors and lung stretch receptors as well as a discord between central output and amount of airflow.22
The causes of silent hypoxaemia and underlying pathophysiological mechanisms are not clearly understood. There are limited data describing this phenomenon; however, it is thought to stem from initial insult to the lungs caused by the direct effect of the SARS-CoV-2 virus and/or secondary immune system-mediated inflammation.7 The lung insult results in alveolar epithelial and capillary endothelial damage, interstitial oedema and alveolar fluid filling, which are typical features of ARDS.
Silent hypoxaemia from COVID-19 is thought to be due to an atypical form of ARDS because autopsy findings have demonstrated typical pathological features of ARDS.23,24 However, pathophysiological differences exist between ARDS that is associated with COVID-19 and ARDS from other causes, such as the presence of more vascular abnormalities in COVID-19 lung injury.7,25 The vascular abnormalities include micro- and macro-thrombosis, vascular dilation and aberrant angiogenesis, which have also been found in other organs in patients with COVID-19.22,26,27 This supports the notion that COVID-19 is part of a systemic vascular pathological process.25
Various theories have been proposed to explain the underlying mechanisms causing silent hypoxaemia in COVID-19. These reflect changes that may occur in the lung parenchyma, blood vessels and neural centres of ventilation control, although the evidence to support them is conflicting. Due to the lack of data in this novel disease, some of this evidence is based on the pathophysiological mechanisms that are known to occur in ARDS due to other causes.7
In non-COVID-19 ARDS, pathological changes result in the lungs becoming more stiff (i.e. lung compliance is reduced). In contrast, the pathological lung changes observed in COVID-19 related ARDS may result in normal or minimally reduced lung compliance.9,28-30 This is somewhat surprising, given the changes of focal and/or bilateral peripheral ground glass opacification and/or consolidation shown on chest imaging in these patients.14 Minimal changes to lung compliance in these patients may mean there is a smaller increase in work of breathing or respiratory drive required to achieve appropriate oxygenation.9,28-32 Additionally, in non-COVID-19 ARDS gas exchange abnormalities can occur as a result of ventilation-perfusion (V-Q) mismatch typically due to fluid filled alveoli or nonventilated areas of lung still being perfused (i.e. shunting). In patients with COVID-19, gas exchange abnormalities may be predominantly due to V-Q mismatch from vascular mediated injury, rather than from injury to the lung parenchyma.7,11 Consequently, lung compliance may not necessarily be affected. However, these theories have not been substantiated because a wide range of changes in lung compliance occur in both COVID-19 and non-COVID-19 related ARDS.7
Impaired pulmonary vascular regulation and vasoplegia (i.e. the absence of hypoxic pulmonary vasoconstriction) is another possible mechanism contributing to silent hypoxaemia.9 Computed tomographic perfusion imaging has shown vascular engorgement and increased perfusion to areas of diseased lung in patients with COVID-19.33 Although this does not provide clear evidence for impairment in hypoxic pulmonary vasoconstriction, it suggests that there may be dysregulation in pulmonary perfusion. Direct effects of the virus on the microvascular endothelial cells may also impair the signals that usually occur in response to hypoxia.34
The SARS-CoV-2 virus can also have direct effects on chemoreceptors involved with neural signalling and ventilation control.35,36 This may lead to impairment of central and peripheral oxygen sensing systems and subsequent loss of dyspnoea sensation.
The postulated mechanisms for direct effects of the virus on the pulmonary vasculature and peripheral and central chemoreceptors may be related to expression of angiotensin-converting enzyme-2 (ACE-2) in these structures, as the SARS-CoV-2 virus has an affinity to bind to the ACE-2 receptor on human cells.2,37 There are very limited data to confirm these theories and further research is required to increase our understanding of silent hypoxaemia in COVID-19.
Management of silent hypoxaemia
The management of silent hypoxaemia rests on recognition and early intervention. With the ability to monitor patient oxygen saturation remotely via pulse oximeter, early detection is feasible, and many outpatient programs provide patients with equipment for self-monitoring.38 Patients with silent hypoxaemia are at risk of rapid deterioration, development of respiratory failure and increased risk of death, therefore early initiation of respiratory support is paramount. Subsequent management of respiratory failure involves support with supplemental oxygen and appropriate noninvasive or invasive ventilation. Concurrent medical management of COVID-19 may incorporate medications such as immunomodulatory therapies, including dexamethasone and tocilizumab, and antiviral agents such as remdesivir.39 Ventilatory techniques, including self-initiated prone positioning in nonventilated patients are widely used, with at least a trend towards benefit being shown in the setting of a randomised controlled trial.40,41
Conclusion
Few clinicians in current practice have had to manage the volume and extent of respiratory failure that COVID-19 has brought about. Even in Australia, which has been relatively protected, the pandemic has stretched resources, including those of intensive care and respiratory medicine. Silent hypoxaemia may be unique to COVID-19 or may represent effects of acute viral pneumonia that have only now achieved widespread recognition. Recognition of this phenomenon in patients with COVID-19 who are in the community is challenging because patients do not report dyspnoea and are not in respiratory distress. The degree of hypoxaemia is out of proportion to their symptoms, or lack thereof, and the use of a simple tool such as a pulse oximeter is an easy way to identify hypoxaemia. An understanding of the possible physiological mechanisms – respiratory, vascular and neurological – will help clinicians detect this condition early, anticipate deterioration, institute therapies and lead to better outcomes and longer-term recovery for patients.
The sheer magnitude of the SARS-CoV-2 pandemic has thrown many aspects of viral disease into sharp relief, ranging from public health measures to innovative developments in intensive care medicine. Silent hypoxaemia, which is crucial to detect and rewarding to treat, may represent just such a phenomenon. RMT