Why should we treat obstructive sleep apnoea?

Heart diseases
Obstructive sleep apnoea is a common condition that has been shown to impact cardiovascular and other health and quality of life outcomes. What have we learned from the recently published SAVE study – the largest intervention study in obstructive sleep apnoea?
Obstructive sleep apnoea (OSA) is a common condition, with symptomatic sleep apnoea affecting 14% of men and 5% of women.1 In addition, OSA has been shown to be associated with increased cardiovascular risk.2 For this reason, it has long been thought that treating OSA with continuous positive airway pressure (CPAP) would negate the cardiovascular risk.
Many studies have shown that in people with OSA, physiological endpoints such as blood pressure or other haemodynamic parameters improve with CPAP treatment, but no studies have shown that using CPAP reduces the rate of future cardiovascular events. This was the impetus for the development of the Sleep Apnea Cardiovascular Endpoints (SAVE) study, the largest intervention study in sleep apnoea undertaken to date.3,4 The SAVE study researchers showed that in people with significant OSA and existing cardiovascular or cerebrovascular disease, treatment with CPAP did not reduce the risk of future events.4 Considering the SAVE study results, it is important to review sleep apnoea treatment and what clinicians hope to achieve by treating sleep apnoea.
What is obstructive sleep apnoea?
OSA is a condition characterised by repetitive narrowing of the upper airway during sleep, resulting in disruption to sleep as well as physiological changes including oxygen desaturation. Not all people with measurable apnoeas during sleep develop clinical symptoms such as sleepiness. When measurable episodes of OSA occur together with symptoms of sleepiness, this is called obstructive sleep apnoea syndrome.
The prevalence of OSA varies depending on how OSA is defined, the testing methods and scoring criteria used, and the apnoea hypopnoea index (AHI) threshold. The AHI is the number of apnoeas or hypopneas recorded per hour of sleep. In a study of middle-aged adults that used a threshold of five or more apnoeas/hypopneas per hour with a desaturation of 4% or greater, the prevalence of OSA syndrome was 4% and 2% in men and women, respectively, whereas OSA without significant symptoms occurred in 24% of men and 9% of women.5
What are the risks and impacts of OSA?
The presence of OSA has been associated with significant health risks and impacts that can be grouped in to three main categories, as discussed below.
Accident risk
The increased sleepiness seen in people with untreated OSA has been associated with higher rates of job-related and motor vehicle accidents.6 Estimates of risk vary depending on the population studied, but range between a two- and tenfold increase in motor vehicle accident risk compared with control groups.7
Impaired neurocognitive function
Individuals with OSA can feel sleepy and unrested and have reduced cognitive function and poorer quality of life.8 Many people with OSA also have depressive symptoms, with 53% of a sample of people referred for assessment of snoring or sleep apnoea having a diagnosis of depression or scoring in the depressed range on validated questionnaires.9
Increased health risk
People with untreated OSA are at increased risk of developing – cardiovascular disease including hypertension, coronary artery disease, congestive heart failure and stroke.2 There are also associations between sleep apnoea and arrhythmias such as atrial fibrillation and metabolic dysregulation, affecting glucose control and risk for diabetes.10,11
Does treating OSA reduce cardiovascular risk?
There have been several small studies showing that sleep apnoea treatment such as CPAP or use of oral appliances (mandibular advancement splints) reduces physiological measures associated with cardiovascular risk, like blood pressure or endothelial function.12,13 These studies led to a belief that treatment of OSA with CPAP must reduce the future risk of cardiovascular events because it reduces surrogate markers or intermediate factors that can lead to cardiovascular events.
Long-term observational studies have also suggested that patients who use CPAP to treat sleep apnoea have a reduced risk of future cardiovascular events compared with those who do not use CPAP.14 However, the observational study design meant that other factors may have contributed to the reduced cardiovascular risk. For example, people who chose to use CPAP may have also looked after other aspects of their health, such as nutrition, physical fitness, weight, blood pressure and cholesterol levels, all of which significantly affect cardiovascular risk.
In contrast, when studies have been designed specifically to look at the effect of OSA treatment on cardiovascular events by randomising patients to CPAP or no CPAP treatment, they have not shown any reduction in future cardiovascular events.15-17 These studies were relatively small, so to assess the effect of CPAP on future cardiovascular events the SAVE study was conducted.4
What was the SAVE study?
The SAVE study was designed as a secondary prevention trial in adults with existing cardiovascular disease and moderate to severe sleep apnoea. The aim of the study was to see whether treatment with CPAP reduced the future risk of serious cardiovascular events. To answer this question, 2717 adults between the ages of 45 and 75 years with moderate to severe obstructive sleep apnoea and existing coronary or cerebrovascular disease were randomised to treatment with CPAP plus usual care or to usual care alone.3 This large number of subjects makes the SAVE study the largest intervention study in sleep apnoea to be undertaken to date.
In the SAVE study, moderate to severe sleep apnoea was diagnosed if at least 12 respiratory events occurred with an oxygen desaturation of 4% or more per hour during a sleep study that measured nasal airflow, respiratory effort and oxygen saturation.3 Participants were excluded if they had very severe hypoxaemia (oxygen saturation below 80% during more than 10% of the night) or severe excessive sleepiness (Epworth Sleepiness Score above 15). Study participants were followed for an average of 3.7 years.
What did the SAVE study show?
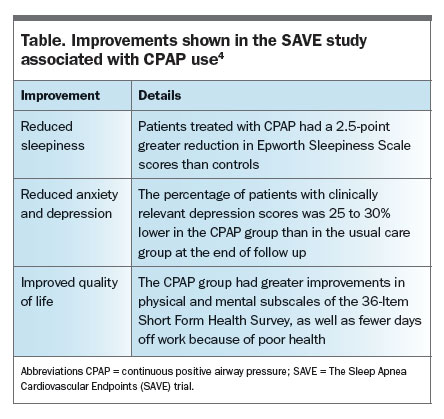
The primary endpoint of the SAVE study was the rate of cardiovascular events. In those treated with CPAP, 17% had a cardiovascular event during the average 3.7-year follow up, compared with 15.4% of those not treated with CPAP. Although the SAVE study did not show a reduction in cardiovascular events, there were factors which may have led to underestimation of the effect of CPAP, such as poor adherence with CPAP and relatively short follow up (3.7 years). Therefore, the SAVE study may not be the final answer on the role of CPAP in reducing future cardiovascular events. Even though cardiovascular events were not reduced, there were significant improvements in sleepiness, anxiety, depression and quality of life (Table).
{kind=link}
Why should OSA be treated?
Considering the SAVE study results, the focus of sleep apnoea treatment should be on managing symptoms and their associated impact on sleepiness, mood, quality of life and accident risk. The SAVE study and other studies have shown that treating people with moderate to severe OSA with CPAP improves these important outcomes.4,18 Although CPAP was the treatment used in the SAVE study, other treatments for OSA, such as oral appliances (e.g. mandibular advancement splints) or, in selected patients, surgery, are alternative treatment options. A randomised, crossover study of people with mild to moderate obstructive sleep apnoea (five to 30 apnoeas/hypopneas per hour) conducted in Australia showed that symptoms of OSA were equally well controlled with CPAP and mandibular advancement splints.19
There are also health risks that were not assessed by the SAVE study, such as arrhythmia and metabolic dysfunction, which may be improved with CPAP. The SAVE study was a secondary prevention study undertaken in people with existing cardiovascular or cerebrovascular disorders. Given this, the role of treating OSA as a primary prevention measure is not clear. It is important that decisions about whether to treat people with moderate to severe sleep apnoea are made with consideration of an individual’s overall health and comorbidities.
What is a clinical approach to managing patients with OSA?
Asymptomatic OSA
For patients with OSA but no symptoms, rather than focusing on sleep apnoea treatment, the focus should be on reducing overall cardiovascular and cerebrovascular risk by managing other known risk factors such as weight, fitness, blood pressure and cholesterol. However, there will be asymptomatic patients with comorbidities that can be impacted by untreated sleep apnoea, such as arrhythmia. These patients may benefit from treatment of OSA, so decisions about treatment should be individualised and discussed in the light of a person’s overall health and comorbidities.
OSA syndrome
For patients with symptoms of OSA, a trial of CPAP or other sleep apnoea treatments should be offered. This could be considered a trial of treatment, to allow patients and their healthcare providers to assess what benefits they derive from treatment. Decisions about ongoing treatment can then be made taking into account the symptomatic response. Addressing other factors such as weight loss and exercise are also important, but often symptoms of tiredness or sleepiness need to be managed before patients can successfully work on weight and physical fitness.
Severe OSA
For patients with severe OSA and marked hypoxaemia (oxygen saturation less than 80% during more than 10% of the night), it would be prudent to offer CPAP treatment. People with hypoxaemia of this severity were excluded from the SAVE study, so may derive a reduction in future health risk with CPAP, and are at higher risk of cardiovascular events.
Drivers and fatigue-critical occupations
Commercial drivers or people working in fatigue-critical occupations should be considered differently. Among this group of people, self-reported sleepiness is often less frequent than in other groups, so it is not always a reliable indicator of symptoms.20 Given the increased accident risk associated with moderate to severe OSA, treatment should be considered in this group and, in individual cases, there may also be a need for objective vigilance testing, using a tool to measure a person’s alertness.
Conclusion
OSA is a common condition that can significantly impact health, accident risk and quality of life. It is important to identify patients with OSA so treatment can be considered depending on the impact the condition is having and patient-specific characteristics. It is also important to recognise that a diagnosis of OSA identifies an individual as having an increased risk of cardiovascular and cerebrovascular events. Other risk factors for cardiovascular disease should be managed carefully in patients with OSA irrespective or whether or not they go on to specific sleep apnoea treatment. RMT
COMPETING INTERESTS: None.
References
- Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 2013; 177: 1006-1014.
- Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the sleep heart health study.Am J Respir Crit Care Med 2001; 163: 19-25.
- Antic NA, Heeley E, Anderson CS, Luo Y, Wang J, Neal B, et al. The sleep apnea cardiovascular endpoints (SAVE) trial: rationale, ethics, design, and progress. Sleep 2015; 38: 1247-1257.
- McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med 2016; 375: 919-931.
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep disordered breathing among middle-aged adults. N Engl J Med 1993; 328: 1230-1235.
- Jackson ML, Howard ME, Barnes M. Cognition and daytime functioning in sleep-related breathing disorders. Prog Brain Res 2011; 190: 53-68.
- George CF. Sleep apnea, alertness, and motor vehicle crashes. Am J Respir Crit Care Med 2007; 176: 954-956.
- Akashiba T, Kawahara S, Akahoshi T, et al. Relationship between quality of life and mood or depression in patients with severe obstructive sleep apnea syndrome. Chest 2002; 122: 861-865.
- Douglas N, Young A, Roebuck T, et al. Prevalence of depression in patients referred with snoring and obstructive sleep apnoea. Intern Med J 2013; 43: 630-634.
- Stevenson IH, Teichtahl H, Cunnington D, Ciavarella S, Gordon I, Kalman JM. Prevalence of sleep disordered breathing in paroxysmal and persistent atrial fibrillation patients with normal left ventricular function. Eur Heart J 2008; 29: 1662-1669.
- Lam JC, Mak JC, Ip MS. Obesity, obstructive sleep apnoea and metabolic syndrome. Respirology 2012; 17: 223-326.
- Iftikhar I, Valentine C, Bittencourt L, et al. Effects of continuous positive airway pressure on blood pressure in patients with resistant hypertension and obstructive sleep apnea: a meta-analysis. J Hypertens 2014; 32: 2341.
- Schwarz EI, Puhan MA, Schlatzer C, Stradling JR, Kohler M. Effect of CPAP therapy on endothelial function in obstructive sleep apnoea: a systematic review and meta-analysis. Respirology 2015;20(6):889-95.
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005; 365:1046-1053.
- Barbé F, Durán-Cantolla J, Sánchez-de-la-Torre M, et al. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: a randomized controlled trial. JAMA 2012; 307: 2161-2168.
- Parra O, Sánchez-Armengol A, Bonnin M, et al. Early treatment of obstructive apnoea and stroke outcome: a randomised controlled trial. Eur Respir J 2011; 37: 1128-1136.
- Peker Y, Glantz H, Eulenburg C, Wegscheider K, Herlitz J, Thunström E. Effect of positive airway pressure on cardiovascular outcomes in coronary artery disease patients with nonsleepy obstructive sleep apnea. The RICCADSA randomized controlled trial. Am J Respir Crit Care Med 2016; 194: 613-620.
- Dang D, Cunnington D. Sleep apnoea: impact on safety and psychosocial functions. Indian Journal of Sleep Medicine 2009; 4: 95-9.
- Barnes M, McEvoy RD, Banks S, Tarquinio N, Murray CG, Vowles N, Pierce RJ. Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med 2004; 170: 656-664.
- Sharwood LN, Elkington J, Stevenson M, et al. Assessing sleepiness and sleep disorders in Australian long-distance commercial vehicle drivers: self-report versus an ‘at home’ monitoring device. Sleep 2012; 35: 469-475.