Management of COVID-19: practical tools and tips for GPs

COVID-19
Infectious diseases
The COVID-19 pandemic has posed significant challenges to the Australian healthcare system and our society. GPs by necessity have been tasked with reviewing and managing large numbers of patients with COVID-19. This article summarises important information GPs need to effectively assess and manage patients with COVID-19, and provides online ‘living’ resources to help them keep up to date.
- GPs are often the first point of call for patients with coronavirus disease 2019 (COVID-19) in the community and are well placed to co-ordinate their recovery after infection.
- COVID pneumonia is the major cause of mortality in patients with acute infection.
- The severity of acute COVID-19 determines overall management.
- Disease-modifying treatments are available for certain populations to reduce the risk of severe disease.
- Evolving virus variants will affect the effectiveness of treatments.
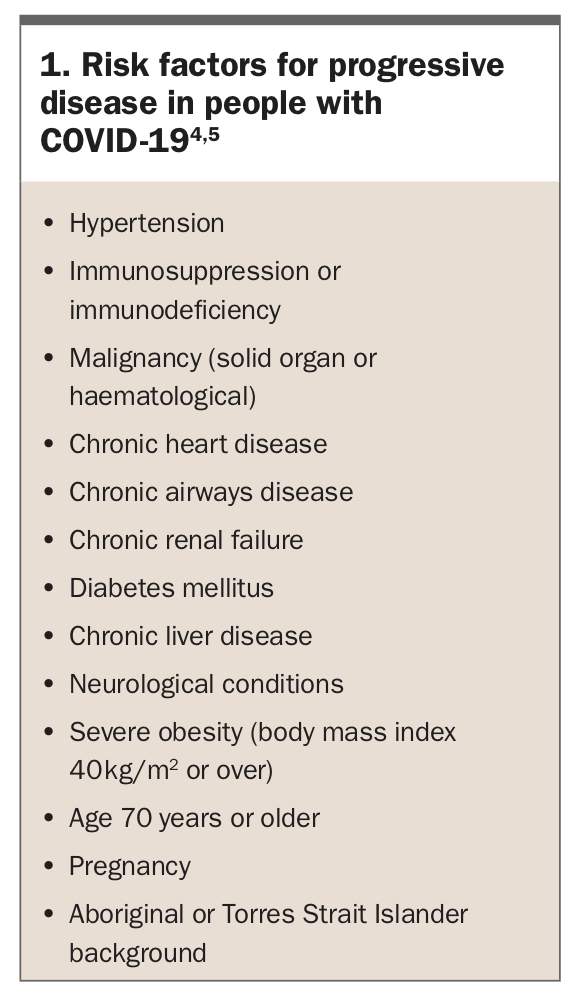
Coronavirus disease 2019 (COVID-19) has swept the globe. At the time of writing, more than 4 million infections with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and more than 6000 deaths have been reported in Australia.1 Most people with COVID-19 experience mild symptoms and make a full recovery.2,3 However, some develop moderate to severe respiratory symptoms and signs of COVID pneumonia and require specialised care, usually provided by tertiary care hospitals. Risk factors for developing moderate to severe disease are summarised in Box 1.4,5
{kind=link}
Compared with common seasonal viral illnesses, SARS-CoV-2 infection has a much higher incidence of lower respiratory tract infection. This can lead to marked hypoxia and acute respiratory distress syndrome, the major cause of mortality in patients with COVID-19.6 In patients who require hospitalisation, the average time from first symptom to dyspnoea is five days, with the median time to intubation and mechanical ventilation being 8.5 days.7 It is important to identify patients with COVID pneumonia and those at high risk of deterioration.
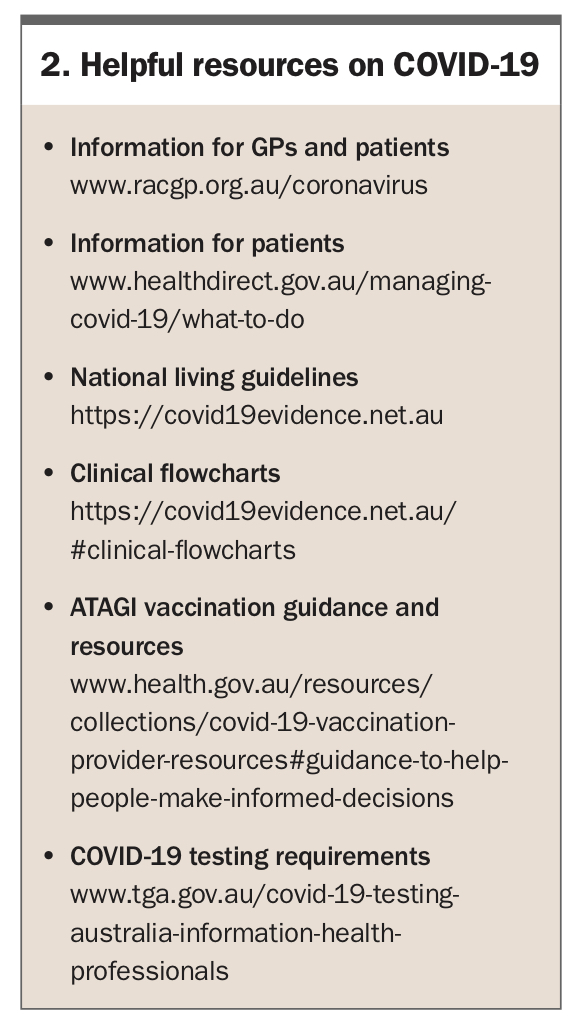
This article discusses the assessment and management of patients with COVID-19 in general practice. Given the relatively short duration of the pandemic, evidence is evolving rapidly and information may quickly go out of date. We therefore also provide resources to help medical practitioners keep up to date (Box 2). These include the living guidelines of the National COVID-19 Clinical Evidence Taskforce (https://covid19evidence.net.au). These guidelines have been developed by a multidisciplinary group of researchers and clinical experts and are updated regularly.8 They include easy-to-follow flowcharts for the current evidence-based management of COVID-19.
{kind=link}
How to assess disease severity and why is this important?
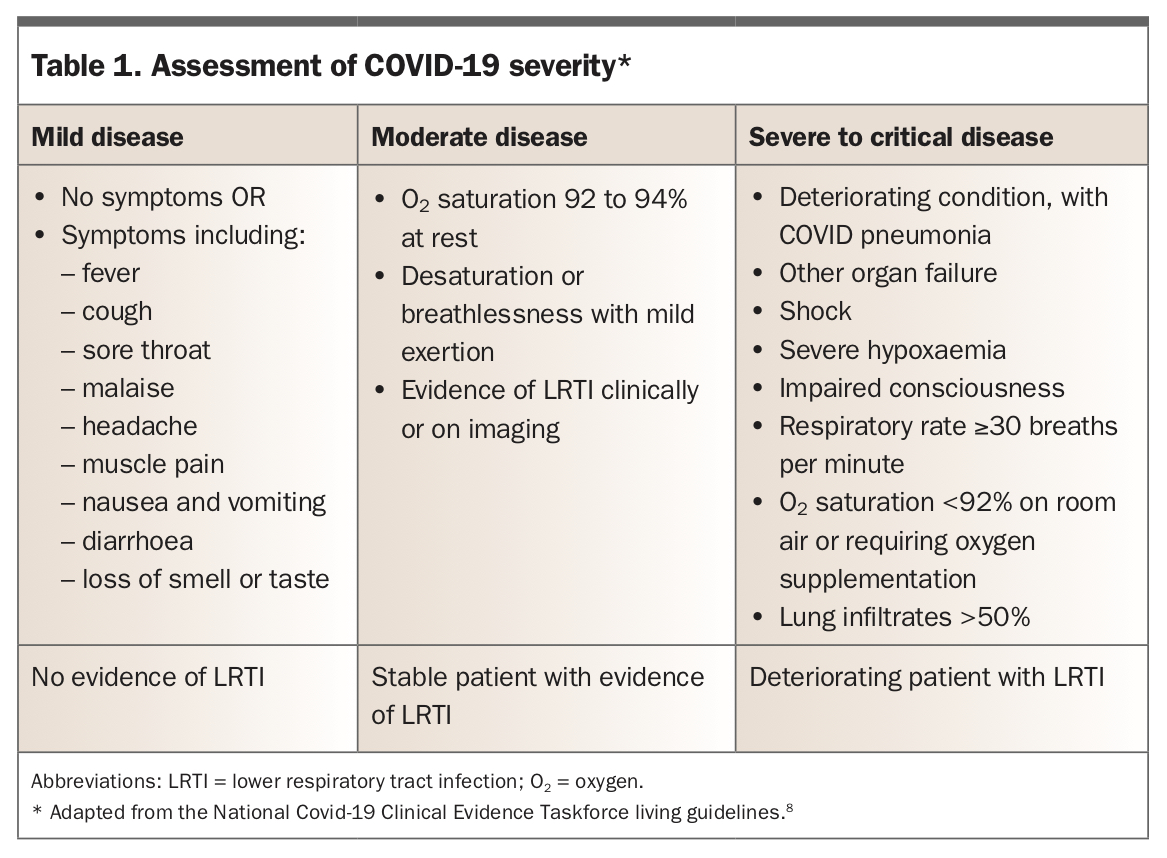
An understanding of both disease severity and the natural history of COVID-19 is paramount to COVID-19 management. Features indicating disease severity are summarised in Table 1.8 Delayed identification and referral to hospital for COVID pneumonia are associated with higher mortality and poorer outcomes.9
{kind=link}
For primary healthcare professionals, most clinical assessments occur via telehealth (by video or telephone). Key points to note in the patient’s history include:
- vaccination status
- date of symptom onset
- severity of symptoms
- risk factors for progression and severe disease
- presence of sick contacts and home circumstances
- which test was performed for diagnosis: rapid antigen test (RAT) or polymerase chain reaction (PCR) test.
PCR is the ‘gold standard’ for COVID-19 testing, but RATs allow for more timely results at the cost of lower sensitivity, particularly if a person is asymptomatic. Patients who are symptomatic and have a negative RAT result should be encouraged to have a PCR test.10 The TGA website includes links to current recommendations on COVID-19 testing by state or territory and local health network (www.tga.gov.au/covid-19-testing-australia-information-health-professionals).10
Symptoms of mild illness may include any of the following: fever, cough, sore throat, loss of smell or taste, nausea and vomiting, diarrhoea, headache and muscle pains. Symptoms that suggest worsening infection include dyspnoea, confusion, significant fatigue, persisting fever, chest tightness, abdominal pain, diarrhoea and vomiting. Of these, dyspnoea remains the strongest predictor of disease progression.9
An important consideration for monitoring patients with COVID-19 is to suggest or supply a pulse oximeter to measure oxygen saturation. Oxygen saturation is the most consistent indicator of disease severity in adults. Symptoms may not always be present with disease progression, or conversely hypoxia is not always present in patients with dyspnoea.11 Pulse oximetry allows for close monitoring as some patients can exhibit ‘silent hypoxia’, having minimal to no symptoms with oxygen saturations less than 95%.9,12,13
In addition to assessing respiratory status, it is important to consider an individual’s social situation, particularly their ability to self-isolate, self-monitor and manage at home. An inability to do so may warrant a higher level of support.
The management of COVID-19 is ultimately determined by the severity of disease. Patients with mild disease can typically be managed in the community, whereas those with moderate to critical disease are managed in hospital.
Who can be managed in the community?
Most healthy patients with mild symptoms require supportive management only and can be managed well in the community. Patients can be directed to resources that help them monitor their own symptoms. Healthdirect has developed an online tool that provides information for patients when they test positive for COVID-19 (www.healthdirect.gov.au/managing-covid-19/what-to-do).
Disease-modifying agents
Most patients who develop COVID-19 will not benefit from disease-modifying agents. Selected patient groups who are most likely to benefit from these therapies include:
- people who are immunocompromised
- those who are partially vaccinated or unvaccinated
- patients most at risk of disease progression.
Resources such as the National COVID-19 Clinical Evidence Taskforce guidelines give specific details on each medication and the patient groups most at risk of disease progression.14 Disease-modifying agents should be commenced early within the first five to seven days after symptom onset. As such, early diagnostic testing is recommended. These disease-modifying treatments have been shown to reduce the risk of subsequent hospitalisations and mortality.14 It is important for all primary care health professionals to be aware of the referral pathways in their local health network to access these therapies.
Inhaled corticosteroids
Inhaled corticosteroids are easily accessible and provide a possible benefit to patients with COVID-19 who do not require supplemental oxygen and are in the first 14 days of infection. Inhaled corticosteroids are suggested for people with diabetes, heart disease, asthma or lung disease, immunosuppression, mild hepatic impairment, stroke or neurological problems. Formulations include budesonide or ciclesonide.14
Sotrovimab
Sotrovimab is a novel monoclonal antibody that targets the spike protein of SARS-CoV-2. It is available for use by regulatory approval for patients with mild to moderate COVID-19 who do not have adequate immunity to COVID-19 (e.g. they are undervaccinated or immunosuppressed). Treatment involves a single intravenous infusion delivered over one hour.14
In the COMET-ICE trial, sotrovimab reduced the risk of hospitalisation or death by 85%.15 Preprint studies suggest that the Omicron BA.2 subvariant exhibits marked resistance to sotrovimab.16
Casirivimab plus imdevimab
Casirivimab plus imdevimab is a novel monoclonal antibody that has reduced efficacy against the Omicron variant of SARS-CoV-2 and will not be discussed further here. Details of this medication are available in the National COVID-19 Clinical Evidence Taskforce guidelines.8
Molnupiravir
Molnupiravir is an oral antiviral agent that should be commenced in the first five days of COVID-19 illness. It is taken every 12 hours for five days, with or without food. Given the oral formulation, it can be used in patients who would struggle to attend a COVID care centre, particularly residents of aged care facilities, and the Australian Government has pre-placed molnupiravir in some residential aged care facilities.
On 1 March 2022, the PBS listed molnupiravir for the treatment of COVID-19 in:17
- individuals aged 65 years or over and at high risk (defined as at least two high-risk features, which include fewer than two doses of SARS-CoV-2 vaccine, age 75 years or over, in residential aged or disability care and specific comorbidities)
- Aboriginal or Torres Strait Islander people aged 50 years or over and at high risk (defined as above)
- people aged over 18 years who are moderately to severely immunocompromised.
Molnupiravir should not be used in people with severe renal or liver impairment. It is contraindicated during pregnancy and breastfeeding. Sexually active patients with childbearing potential require appropriate contraception if given molnupiravir. Effective contraception should be continued for four days after the final dose of molnupiravir for women and three months after the final dose for men. Molnupiravir is a prodrug of N-hydroxycytidine, which in high doses in animal models has been linked with fetal lethality and teratogenicity.18
The safety and efficacy of molnupiravir was assessed in the MOVe-OUT trial, which was stopped early. Overall, there was a relative risk reduction (RRR) of 31% (absolute risk reduction 3.0%), although the initial press release quoted a RRR of almost 50%.19 There is concern that truncating the trial may have led to an overestimation of the effect size. Common adverse reactions include diarrhoea, nausea and dizziness.19 Another limitation of molnupiravir is the significant cost of the medication to the Government, at over $900 per course.20
Nirmatrelvir plus ritonavir
Nirmatrelvir plus ritonavir is an oral antiviral agent that is administered every 12 hours for five days. The EPIC-HR trial showed an RRR for hospitalisation or death of 89%.
Nirmatrelvir targets a protease enzyme of SARS-CoV-2 and is metabolised mainly by the cytochrome isoenzyme CYP3A. Coadministration with low-dose ritonavir, a strong inhibitor of CYP3A, increases plasma concentrations of nirmatrelvir.21 This combination medication has many significant drug interactions, particularly with direct oral anticoagulants, some antiarrhythmics, antipsychotics and some statins.22 It is crucial to check for drug interactions before prescribing because of the heightened risk of drug toxicity.
Women with childbearing potential should be advised to use effective contraception for the duration of treatment. Ritonavir may reduce the efficacy of the combined oral contraceptive pill.14 Alternative methods of contraception, including barrier contraception, should be considered.
Chemoprophylaxis
The National COVID-19 Clinical Evidence Taskforce guidelines provides further information on postexposure prophylaxis. However, currently with the dominance of the Omicron variant, no highly efficacious medication exists for postexposure prophylaxis.
Who should be referred for further evaluation?
It is important to consider referring patients with signs or symptoms of moderate to severe COVID-19 for in-person review. The appropriate referral site depends on symptom severity as follows.
- Patients with an oxygen saturation of 90 to 94% or dyspnoea on mild exertion can be referred to a COVID-19 referral centre.
- Referral to an emergency department is warranted for patients with severe dyspnoea (occurring at rest), oxygen saturation of 90% or less, altered mental state, symptoms of hypoperfusion (low urine output or collapse) or symptoms indicating significant complications, such as acute coronary symptoms.
If there is concern about a patient’s overall clinical state, GPs should not hesitate to refer. Patients can deteriorate rapidly, and delayed presentation to hospital has been associated with worse outcomes.9
Various inpatient disease-modifying treatments are available, including dexamethasone, remdesivir, tocilizumab and baricitinib. However, not all patients are prescribed these. Evidence suggests that corticosteroids have the greatest benefit in patients who require supplemental oxygen.23 In contrast, remdesivir is used in hospitalised patients with or without supplemental oxygen, but should not be used in those who require ventilation, either noninvasive or invasive. Baricitinib and tocilizumab are reserved for those with progressive deterioration.14
What is Omicron and how does it change management?
The WHO defines a SARS-CoV-2 variant of concern as a variant which shows increased transmissibility, increased virulence, a change in clinical disease presentation or decreased effectiveness of public health measures, vaccines and therapeutics.24 The most recent variant of concern is the Omicron variant, which was first documented in November 2021.24
Modelling suggests that Omicron has a 13-fold increase in infectivity compared with the original virus and is 2.8 times more infectious than the Delta variant.25 Early outbreak investigations suggest that the median incubation period is three days.7,26 Study data released by King’s College London and the health science company Zoe suggest the top five symptoms of the Omicron variant are a runny nose, headache, fatigue, sneezing and sore throat. Loss of smell or taste is not as prevalent as for the Alpha variant.27
Observation of disease caused by the Omicron variant shows an increased incidence of reinfections and breakthrough infections despite two or three doses of mRNA vaccine. In-vitro studies show the level of neutralising antibodies is lower against Omicron compared with other variants after two doses of vaccine, with the level increasing after a third dose of vaccine.28 Reports suggest that some disease-modifying treatments, such as bamlanivimab and casirivimab-imdevimab, have reduced efficacy against the Omicron variant.29
In recent weeks, infections caused by the BA.2 subvariant of Omicron are increasing relative to the ‘original’ BA.1 subvariant. Initial data suggest that BA.2 is more transmissible than BA.1, although the increase is less than that for BA.1 compared with Delta. Infection with BA.1 seems to have a strong protective effect against BA.2; however, reinfection with BA.2 has been documented.30
Ultimately, as the pandemic continues, mutations will accumulate, creating new variants. This will challenge current therapeutics and vaccines, requiring our response to evolve.
Special patient groups
People with pre-existing cardiac or respiratory disease
People with comorbid cardiopulmonary disease are at higher risk of moderate to severe COVID-19, particularly those with heart failure and chronic obstructive pulmonary disease. Patients with cardiopulmonary disease have a lower functional reserve, and an insult such as COVID-19 can have a far greater impact on their overall function. Additionally, those with severe cardiopulmonary disease may already have breathlessness on exertion, making it difficult to assess a change from their usual baseline symptoms.
Ultimately, it is important to ensure that this patient group is closely monitored. Patients who are already receiving long-term oxygen therapy for cardiopulmonary disease or have known hypercapnia due to ventilatory failure may have lower oxygenation targets; however, there is also a risk of underappreciating the severity of disease. It is difficult to give specific targets for these patients as each will have a different target. Careful review of oximetry in these patients is important, and community-based practitioners should not hesitate to engage in early discussion with cardiac and respiratory specialists about these patients.
Data regarding the risk of severe COVID-19 and asthma are conflicting. Some studies report higher risk, whereas others suggest lower risk.31,32 Patients with asthma have a reduced expression of ACE-2 receptors in airways, suggesting a plausible biologic explanation for reduced risk.33 Despite the conflicting data, it is important that patients with asthma have an up-to-date asthma action plan and maintain adherence to their prescribed medication and good inhaler technique. In general, until stronger evidence is obtained, patients with asthma should continue to take precautions, practise social distancing and be up-to-date with vaccination.
Another consideration for patients with asthma is whether their symptoms are related to COVID-19 or an infective exacerbation of asthma. We and other practitioners have noted patients who are concerned about their asthma control in the setting of acute COVID-19. Some patients who have not required reliever inhalers for years have been prone to overusing them for COVID-19-related symptoms. Despite not obtaining a symptomatic benefit, they have continued to use reliever inhalers because of concern about an asthma exacerbation. Because of the difficulty of differentiating between an acute asthma exacerbation and COVID-19 symptoms via telehealth, we recommend that GPs consider discussing patients with asthma and COVID-19 with a COVID-19 referral centre or respiratory specialist colleague if they have any concerns.
Pregnant women
Pregnant women do not seem to be more susceptible to COVID-19 but are at higher risk of adverse outcomes (Table 2).34,35 Among neonates of women who tested positive for COVID-19, 13% also tested positive.35 The risk of more severe illness and pregnancy-related complications appears increased for both the mother and neonate, particularly if the infection occurs in the third trimester.36
{kind=link}
Vaccination is safe during pregnancy and also significantly reduces the risk of COVID-related complications. Compared with unvaccinated women, vaccination is not associated with preterm birth or small-for-gestational-age at birth.37 Vaccination reduces admission rates to both hospital and the intensive care unit.34
In general, the risk of venous thromboembolism (VTE) is higher in pregnant women than in the general population. This risk increases further in the setting of acute COVID-19. For pregnant women who are isolating at home and have no further risk factors for VTE, prophylactic enoxaparin or heparin is not recommended.38 However, for women with further risk factors, including but not limited to hospitalisation, obesity, pre-eclampsia or multiple pregnancies, pharmaceutical prophylaxis could be considered, ensuring there are no other contraindications.39 Further risk factors can be sought from local or jurisdictional guidance. Prophylactic enoxaparin or dalteparin is preferred and should be continued for a minimum of 14 days or until COVID-19 symptoms have resolved.38 Further considerations for VTE prophylaxis, including dosing, can be found in the National COVID-19 Clinical Evidence Taskforce guidelines.38
There are some important considerations regarding disease-modifying treatments during pregnancy. If tocilizumab is used during pregnancy after 20 weeks of gestation, live vaccines should be avoided in the first six months of the newborn’s life. The National COVID-19 Clinical Evidence Taskforce guidelines provide more detailed information regarding pregnancy and disease-modifying treatments.14
Children
Most children with COVID-19 develop milder disease than adults. US and UK population studies show that severe infection disproportionately affects children with comorbidities and those from minority ethnic groups, which raises concern for Aboriginal and Torres Strait Islander children.40 The criteria for assessing disease severity in children and adolescents differ from those used for adults. Assessment should include feeding, hydration, conscious state, vital signs and work of breathing, with less emphasis on oximetry. The National COVID-19 Clinical Evidence Taskforce flowcharts for children and adolescents provide useful guidance.41
Severe COVID-19 complications can occur in paediatric populations. A known association is paediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS), a hyperinflammatory condition thought to be due to a dysregulated immune response in the postinfectious period.42 Patients present with fever and single or multiorgan dysfunction. Prompt recognition and referral to a paediatric tertiary centre is important to improve outcomes.42 The National COVID-19 Clinical Evidence Taskforce living guidelines have further information on PIMS-TS.43
An issue in management of COVID-19 in the paediatric population is that children are usually excluded from clinical trials. Therefore, most evidence has been extrapolated from adult population studies.14
Immunocompromised patients
People living with HIV or malignancy, transplant recipients and patients taking immunosuppressants often lack the ability to mount an appropriate immune response. Immunocompromised patients are more at risk of severe and prolonged SARS-CoV-2 infection. Even with appropriate vaccination, immunocompromised individuals are also more likely to have breakthrough infections than those who are immunocompetent; however, the severity of illness is lower in immunocompromised patients who are fully vaccinated than in those not vaccinated.44 A third dose of vaccine is associated with higher levels of neutralising antibodies in immunocompromised patients, and they are recommended to receive a third COVID vaccine dose before a booster dose. The Australian Technical Advisory Group on Immunisation (ATAGI) provides excellent resources and guidance on vaccination for patients who are immunosuppressed.45
Many immunocompromised patients who test positive for COVID-19 are eligible for community-based disease-modifying agents, as described above. These treatments can be accessed through the referral pathways of local health networks.
Acute complications of COVID-19
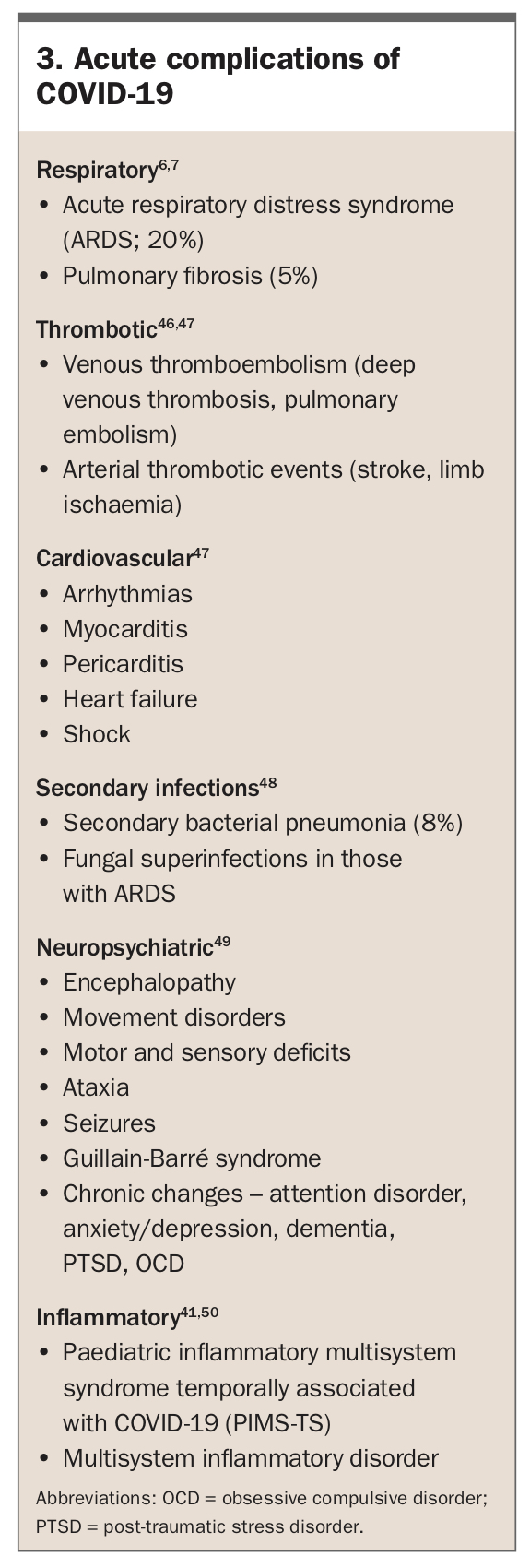
Besides COVID pneumonia, COVID-19 can cause multisystem complications. These include pulmonary embolism, cardiac failure, exacerbation of underlying respiratory disease, myocarditis and myocardial infarction, which are important differential diagnoses for patients presenting with dyspnoea.46,47 Infectious and neurological complications also occur. Potential acute complications of COVID-19 are summarised in Box 3.6,7,41,46-50
{kind=link}
Long COVID
About one-quarter of symptomatic patients with COVID-19 have persistent symptoms for at least one month. One in 10 have persistent symptoms to 12 weeks.51 These symptoms can have a significant impact on function and affect a broad range of systems, including the pulmonary, neurological, psychological and musculoskeletal systems. The most common symptoms include fatigue, headache, dyspnoea and anosmia.52 The exact mechanism of ‘long COVID’ is poorly understood. However, it is more common in women, older patients and those with a higher body mass index.51
Symptoms that require urgent assessment for serious complications include severe or new dyspnoea, hypoxia, syncope, unexplained chest pain, palpitations, arrhythmias, new delirium or focal neurological signs or symptoms. Evidence for managing this post-COVID condition is still emerging.52 Primary care physicians are well situated to co-ordinate patient-centred care with a multidisciplinary team. This may include COVID-specific rehabilitation programs or post-COVID clinics, which many sites have now developed. Access to these should be sought through local health networks.53
Conclusion
GPs are often the first point of call for COVID-positive patients in the community. They have a crucial role in assessing these patients, identifying those who are most likely to benefit from disease-modifying therapies early in the illness course, monitoring for deterioration and referring those with moderate to severe COVID-19 to a COVID-19 referral centre or emergency department. GPs are also well placed to co-ordinate patient-centred care of people with long COVID. RMT