COPD exacerbations. A hearty opportunity

Dr Leong is a Respiratory/Sleep Physician at Monash Health and at Eastern Respiratory Service, Melbourne, Vic.
COPD (chronic obstructive pulmonary disease)
Heart diseases
COPD exacerbations are common. Concurrent cardiovascular involvement is frequent and adversely affects prognosis. COPD exacerbations are opportunities to not only optimise lung health, but also to enhance cardiovascular diagnosis and treatment.
- Chronic obstructive pulmonary disease (COPD) exacerbations are times of physiological stress resulting in heightened cardiovascular risk in individuals at high risk of cardiovascular disease.
- COPD exacerbations can reveal cardiovascular disease and are an opportunity for cardiovascular risk assessment.
- COPD exacerbations are opportunities to make a difference to both pulmonary and cardiac outcomes.
Chronic obstructive pulmonary disease (COPD) affects around one in seven adults over the age of 40 years in Australia and it is anticipated that the prevalence of COPD will rise as the population ages.1 Exacerbations of COPD are impactful events. Exacerbations are typically frightening for patients and signal adverse medical consequences, including accelerated lung function decline and mortality. They are a leading cause of preventable Australian hospitalisations.2
Several lines of evidence point to the critical importance of cardiovascular involvement in COPD exacerbations. For example, cardiac biomarker elevation is detectable in up to 75% of patients who are hospitalised with exacerbations and leads to a greater likelihood of readmission and mortality.3
Large, well-conducted pharmaceutical studies have shown that cardiovascular disease is the most common cause of death in patients with mild and moderate COPD.4
Our research in patients hospitalised with exacerbations of severe COPD has shown that severe cardiovascular disease is commonly present at this time.5 At the clinical level, deaths among patients with severe COPD are more frequently attributed to COPD than to cardiovascular disease, but our data suggest that cardiac involvement may have been underdiagnosed and that cardiovascular intervention could modify outcomes in patients with severe COPD. This article focuses on a practical approach to outpatient cardiovascular disease assessment during and after COPD exacerbation.
COPD-X
Guidelines for COPD management, including exacerbations, are available from COPD-X (www.copdx.org.au), the Australian and New Zealand Guidelines for COPD management. The standard approach to managing exacerbations is outlined in Figure 1. Although cardiovascular assessment is mentioned in the COPD-X guidelines, no specific approach has been outlined.
{kind=link}
There are two key steps in our suggested approach to potential cardiovascular disease in patients with COPD – first, be aware of the possibility of cardiovascular disease in COPD; and second, diagnose and treat cardiovascular disease and/or risk factors (Figure 2).
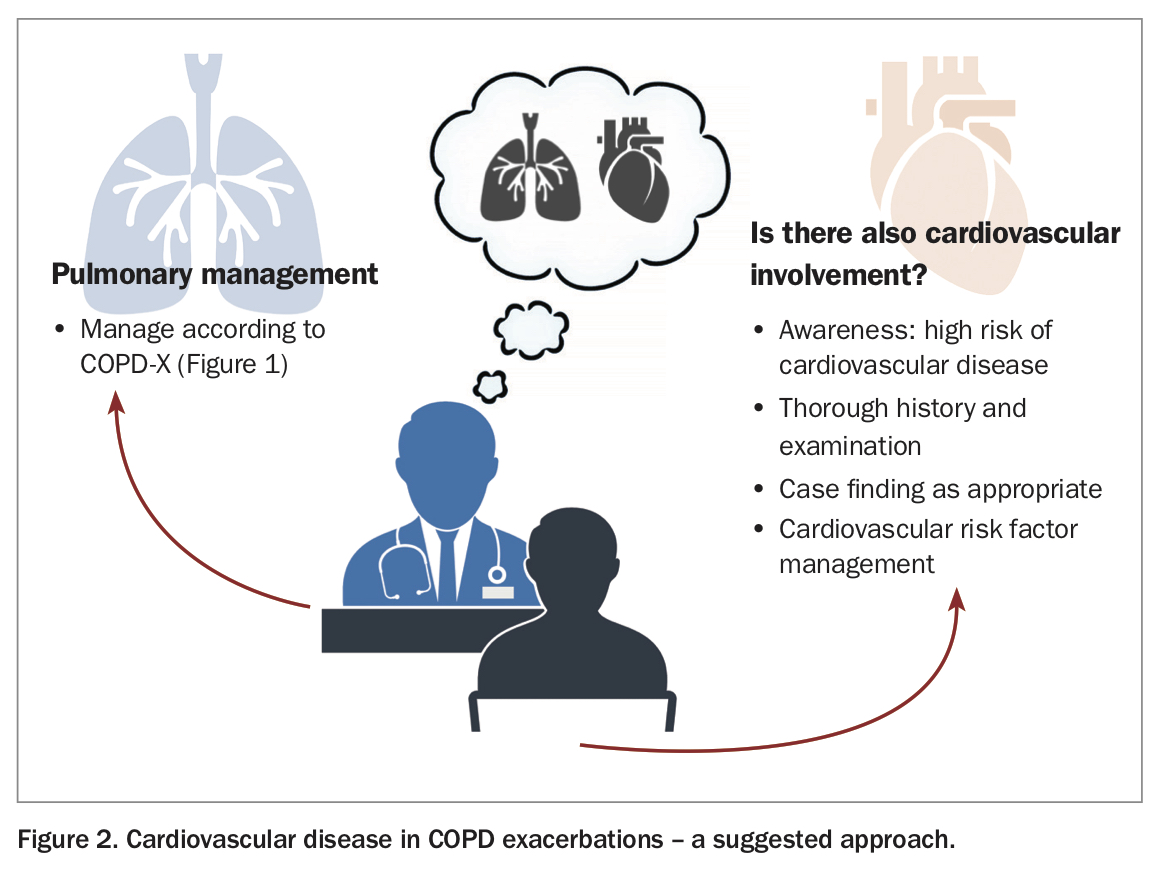{kind=link}
COPD exacerbations and cardiovascular disease
The pretest probability of cardiovascular disease in patients with COPD is often high, as this population is enriched for cardiovascular risk factors. Individuals with COPD are generally older, less physically active and have smoked. By definition, they have airflow limitation, which is an independent cardiovascular risk factor – for every 10% decrease in forced expiratory volume in one second (FEV1), cardiovascular mortality increases by 28%.6 Overall, populations with COPD are at a two- to threefold increased risk of cardiovascular disease compared with controls.7
This underlying cardiovascular vulnerability can be revealed during COPD exacerbations, a time likened to an unstandardised, unscheduled cardiac stress test.8 Cardiovascular event rates, including mortality, spike during exacerbation, and rates remain elevated in the following months.9
Many complex factors can be active separately or together to produce cardiovascular events. Two-thirds of exacerbations are associated with infection (a proinflammatory state), and hypoxia, tachycardia, sudden elevations in pulmonary pressure, arterial stiffness and pulmonary hyperinflation can all contribute to cardiovascular events.3
How does cardiovascular disease present?
Cardiovascular disease during COPD exacerbations may present in the following different ways.3,5
- Cardiovascular disease may mimic a COPD exacerbation. This can masquerade as a ‘refractory’ COPD exacerbation – one which does not respond as expected to standard airway-directed management.
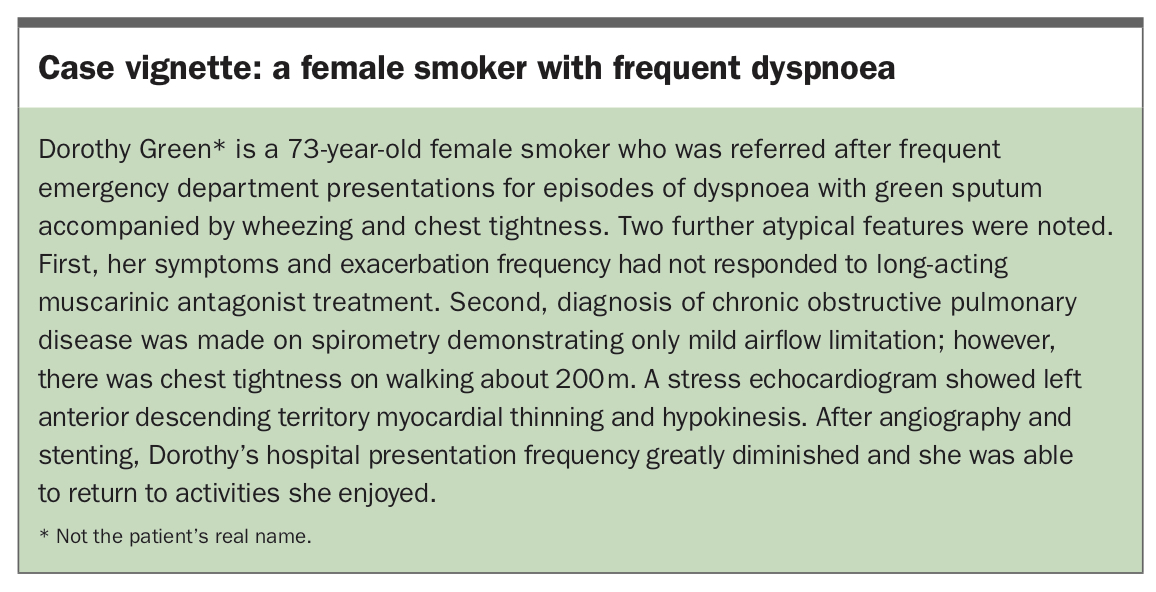
- Cardiovascular disease may diminish the ability of a patient to ‘tolerate’ the exacerbation, and a relatively minor airway disturbance may present with disproportionate or atypical symptoms. A case vignette of a real patient that highlights this is outlined in the Box.
- Cardiovascular disease may complicate COPD exacerbations – a phenomenon exemplified by type 2 (demand) myocardial infarction illustrated by elevated troponin.3
{kind=link}
Diagnosis of cardiovascular disease
Diagnosing cardiovascular disease during COPD exacerbations relies on clinical acumen and a high index of suspicion. This is because manifestations of COPD and cardiovascular disease can overlap and hints may be subtle. For instance, it may be tempting to attribute symptoms including breathlessness, atypical chest pain and tightness to COPD exacerbation; however, cardiovascular disease can present similarly, and careful assessment may yield clues to concurrent cardiovascular disease, addressing questions such as:
- Is there chest pain or tightness and is it exertional?
- Is there a background history of cardiac disease that may be active?
- If this is a first presentation to this practice, does this patient tend to avoid nonacute care, and thus has a greater opportunity for cardiovascular diagnosis and risk factor reduction?
- Are there palpitations?
- Is orthopnoea prominent?
- Is breathlessness out of proportion to spirometric airflow limitation?
The examination can often be helpful. For example:
- blood pressure may be elevated
- radial artery palpation may lead to suspicion of atrial fibrillation, which complicates many exacerbations
- jugular venous pulsation elevation may hint at right heart involvement
- peripheral oedema may hint at cardiac failure
- bilateral basal crackles on auscultation could be a sign of heart failure.
Beyond cardiovascular case finding, COPD exacerbations can be viewed as an opportunity to review cardiovascular risk. Dutch primary care guidelines recommend that cardiovascular risk assessment should be performed in all patients with COPD.10 In a retrospective study of the impact of the new Dutch guideline on cardiovascular risk management in patients with COPD, 90% of patients with COPD were found to be at a high or very high risk of a fatal cardiovascular event (>5% risk over 10 years).10
Our single-centre study indicated that 55% of patients hospitalised with COPD exacerbations have coronary atherosclerosis at a level at which guidelines recommend treatment.5 Although highlighting cardiovascular disease as a comorbidity, Australian and New Zealand guidelines do not make a recommendation for uniform cardiovascular risk assessment in COPD patients. Given the high prevalence of cardiovascular risk factors in patients with COPD, it is sensible to have a low threshold for performing not only case-finding cardiac investigations, but also to consider performing cardiovascular risk factor assessment.
Treatment
Cardiovascular undertreatment is widespread in patients with COPD.8,11-14 Therapies for COPD can impact cardiovascular disease and vice versa.3,8
The acute treatment of COPD exacerbations should follow COPD-X recommendations (Figure 1). Excessive beta-agonist use can lead to lactic acidosis, Takotsubo cardiomyopathy and even myocardial infarction;3,8 therefore, limiting administration to the maximum dose recommended by COPD-X is suggested. This is four to eight puffs of salbutamol (400 to 800 mcg) via metered dose inhaler/spacer every three to four hours. When supplemental oxygen is used, ensuring that oxygen saturations are maintained at 88 to 92% can prevent adverse respiratory and cardiac consequences.15
After recovery, COPD should be managed according to the COPD-X guidelines for stable COPD (https://lungfoundation.com.au/resources/stepwise-management-of-stable-copd). Although recent large studies of inhaled triple therapy combinations (long-acting muscarinic antagonist, long-acting beta agonist, corticosteroid) in patients with COPD showed small reductions in all-cause mortality, the data are not strong enough evidence for recommending escalation of pharmacological treatment to prevent cardiovascular mortality.16,17 Smoking cessation, encouraging a healthy lifestyle that includes exercise and considering pulmonary rehabilitation should be the cornerstones of management and can improve quality of life.
When a patient experiences a COPD exacerbation in the context of a known cardiovascular comorbidity, this is a good opportunity to review cardiovascular reatment. Studies have consistently shown that treatments for major cardiovascular conditions including coronary disease, myocardial infarction and heart failure are routinely underprescribed in populations with COPD. Over half of patients do not receive optimal treatment for these conditions, irrespective of the indication for treatment.5,11,12 Review of treatments may therefore identify a gap that can be resolved to provide genuine therapeutic benefit.
Some therapeutic reluctance has traditionally been present owing to concerns regarding beta-blocker use in COPD; however, beta-blockers are generally safe in patients with COPD, as are aspirin, statins, ACE inhibitors and neprilysin inhibitors.8
When diagnostic and/or therapeutic uncertainty exists (e.g. where asthma overlap is suspected, which might contraindicate beta blocker use), specialist respiratory or cardiac referral could be considered.
Conclusion
COPD exacerbations are opportunities to not only improve respiratory health but also detect cardiovascular disease and optimise cardiovascular health in patients with often significant cardiovascular risk. Astute practitioners can address diagnostic and treatment gaps in both lung and heart health to make a meaningful difference. RMT