Paediatric respiratory health – the importance of taking an environmental history

Asthma in children
Children's health
With asthma and chronic respiratory disease increasingly prevalent in Australia, intervention in early life is imperative to reducing lifelong disease risk. Doctors who treat children should be aware of the consequences of important environmental exposures in childhood and ask about these when appropriate.
- Modern Australian environments contain an increasing variety of chemicals and produce emissions that increase the risk of chronic respiratory disease, yet awareness of these risks is low.
- There is growing evidence that fetal and early-life exposure to air pollutants and other environmental contaminants increase lifelong risk of chronic disease
- Childhood exposure to toxicants can occur from the environment (e.g. contamination of air, water and soil), in the home and at school or childcare (e.g. cleaning and personal care products, candles and incense, and heaters), and ambient air (e.g. bushfires, motor vehicles and industrial emissions).
- Environmental history taking is key to identifying exposures that can increase the risk of chronic disease and exacerbate existing respiratory conditions in paediatric patients.
The global pattern and major causes of disease have changed over recent decades. A recent Lancet Commission on pollution and health showed that pollution, in its broadest sense, was the largest cause of disease and premature death in the world.1 Globally, early childhood deaths and deaths from communicable, maternal, neonatal and nutritional disorders have declined. By contrast, deaths from noncommunicable diseases (NCDs) are increasing, accounting for 70% of all deaths globally today.2,3 A recent landmark decision from a UK coroner listed air pollution as a contributing cause of death in a 9-year-old asthmatic girl.4
The situation in Australia is no different, with a high incidence of chronic disease including obesity, type 2 diabetes, cardiovascular disease, neurobehavioural problems, asthma and chronic obstructive pulmonary disease (COPD). Thirty-one percent of people in Australia report having asthma or chronic respiratory conditions, with an economic cost of $9 billion per annum in direct and indirect costs.5 As asthma and chronic respiratory disease become more prevalent in Australia and the Pacific region, the future costs of diagnosis and treatment will increase dramatically. To alter this trajectory, we need to intervene to reduce exposure to pollutants that cause adverse respiratory outcomes in early life and lifelong disease risk.
Sources of environmental toxicants
Modern Australian environments contain an increasing variety of chemicals and produce emissions that increase the risk of chronic respiratory disease. However, awareness of the risks and avoidable exposures is low, especially in environments in which children spend most of their time in early life (e.g. domestic, preschool care and school). Low awareness among the public, childcare workers, teachers and healthcare professionals contributes to human behaviours that perpetuate and even increase exposures to these pollutants.
Most populations across Australia are exposed to varying amounts of environmental toxicants. Unlike in the USA and UK, Australia has no systematic assessment of environmental exposures and exposure pathways, or the health consequences of these exposures for our domestic population and for that of our regional neighbours. This means that, to some extent, we rely on overseas data. The problem with this is that exposures are very heavily influenced by the environment in which they occur and international data are not always relevant to local conditions.
Exposure to toxicants in childhood
Growing evidence indicates that fetal and early-life exposure to air pollutants and other environmental contaminants increase lifelong risk of chronic disease through mechanisms including endocrine disruption, epigenetic changes and disruption of innate immune defences.6-8 Transplacental transfer, breastmilk, dermal transfer and non-nutritive ingestion result in unique exposure pathways during fetal development and in early life. Young children interact with the environment in their homes and in educational/childcare establishments through breathing air, consuming food and water and through ‘mouthing behaviours’ in which they put their hands, feet and fomites into their mouths, resulting in non-nutritive ingestion of toxicants. Because of their physiological differences, children get a higher ‘dose’ of toxicants from any contaminated environment than do adults.9
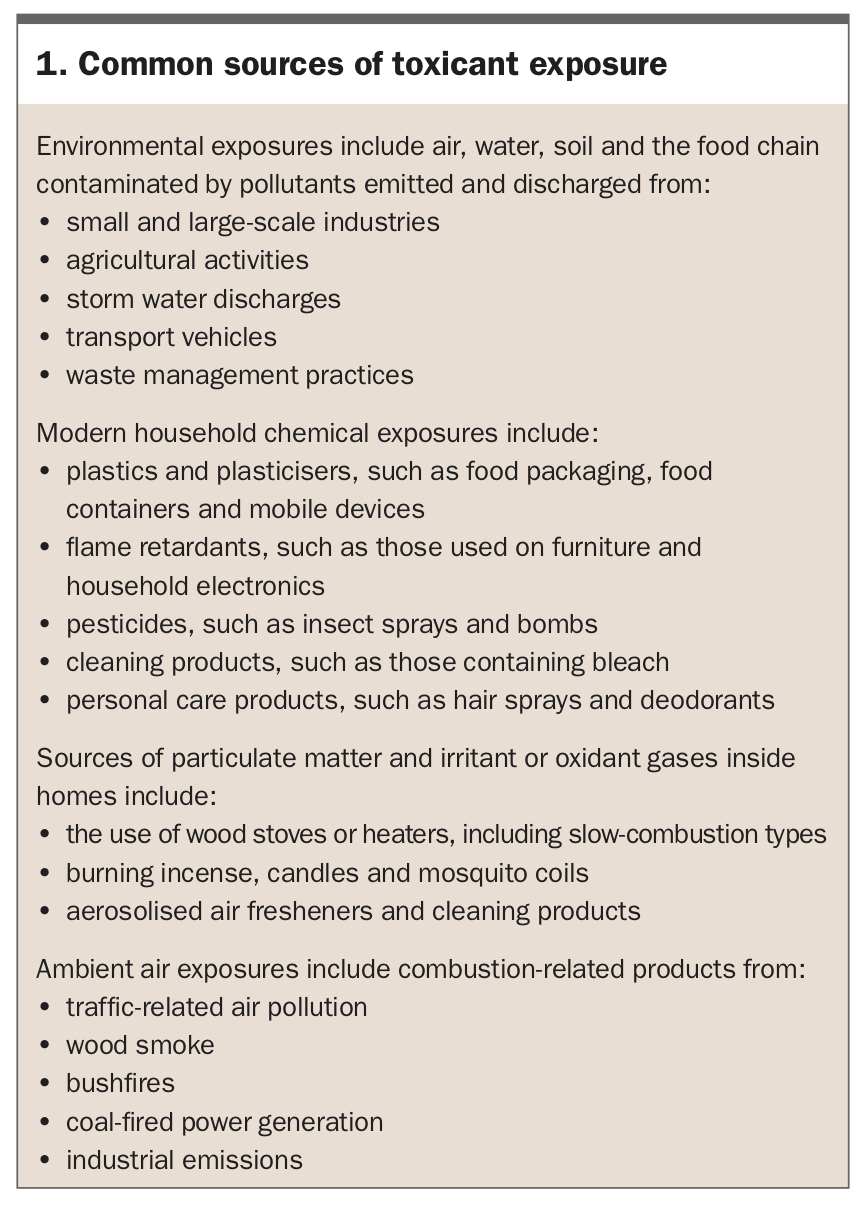
Exposures from the environment, modern household chemicals and ambient air are summarised in Box 1. Environmental exposures can potentially increase exposure to pollutants in communities living or recreating in affected areas, and adverse respiratory health effects from exposure to modern household chemicals have been reported.10-13 Some sources of particulate matter (PM) and irritant or oxidant gases inside homes can emit small particles with mass median aerodynamic diameter below 2.5 microns (PM2.5) that are associated with increased respiratory disease.14-21 Air fresheners and cleaning products, especially those delivered as aerosols, can result in exposures to volatile organic compounds (VOCs) and PM2.5.20,22 Less obvious sources such as burning scented candles also increase VOCs and PM2.5 in indoor environments.19
{kind=link}
Children may also be exposed to toxicants in other environments in which they spend considerable time, such as childcare settings, kindergartens and schools. Family daycare may involve young children spending long periods each day in another home, with all the potential exposures encountered in homes. The use of unflued gas heaters has been a particular problem in some states and territories, and even those labelled ‘low NOx’ heaters, which supposedly emit lower levels of nitrogen oxides, can cause significant respiratory illnesses in exposed children.23 Childcare environments may also have significant sources of VOCs and PM2.5, resulting in increased exposure and poor respiratory health.24 Longitudinal community studies of children exposed to toxic environmental exposures associated with living in the vicinity of the Hazelwood mine fires in Victoria highlight long-term health risks.25
Susceptibility to toxicants in childhood
Not all children are equally susceptible to the health consequences of adverse environmental exposures. The lungs have well-developed defences against irritant and oxidant stimuli, especially those inhaled from the external environment. Many components of the antioxidant defences are under genetic control and low or null-function mutations are relatively common. Individuals with such mutations are more susceptible to the adverse health effects of oxidant particles and gases such as those contained in traffic-related air pollution.26,27 There is some evidence that breastfeeding and dietary or supplemental antioxidants can decrease the adverse respiratory effects of traffic-related air pollution.28 However, much of this evidence is not of sufficient strength to actively advocate the widespread use of antioxidants in all patients.
Environmental exposure history
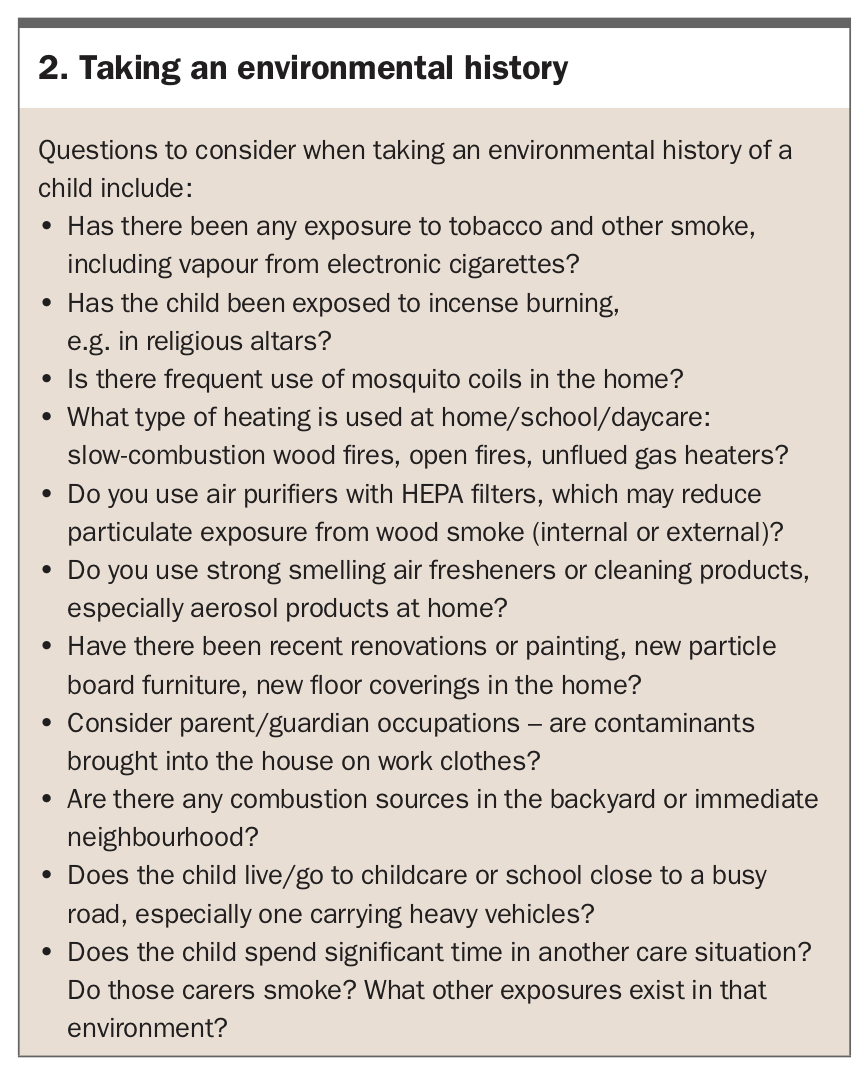
Given this background, what is the relevance for GPs and what should they do in everyday practice? GPs are already aware of the importance of asking patients about cigarette exposure, especially when dealing with children with respiratory disease. This is one simple example of taking an ‘environmental exposure’ history, as outlined in Box 2. As should be evident from the discussion above, taking an environmental exposure history needs to go further than simply asking about smoke exposure.
{kind=link}
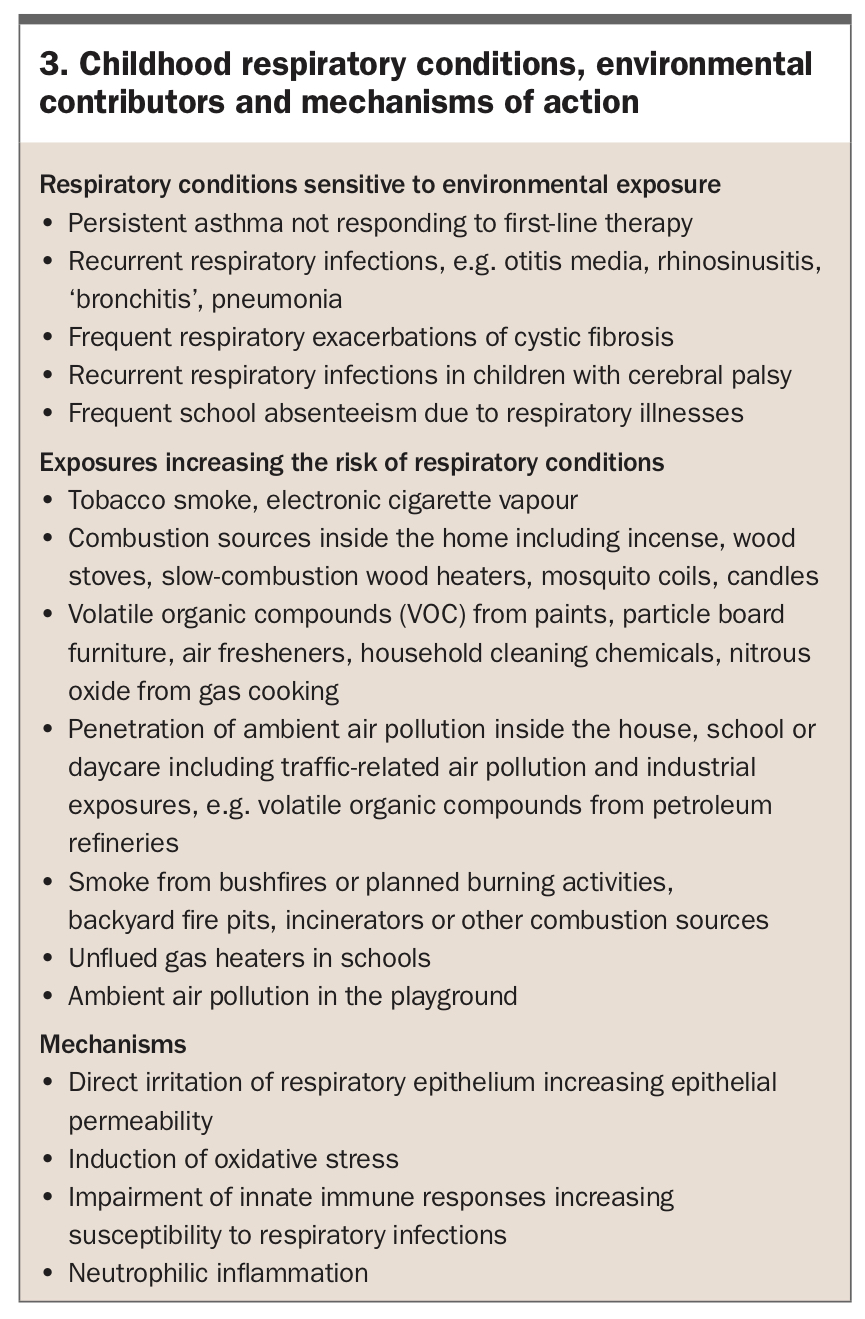
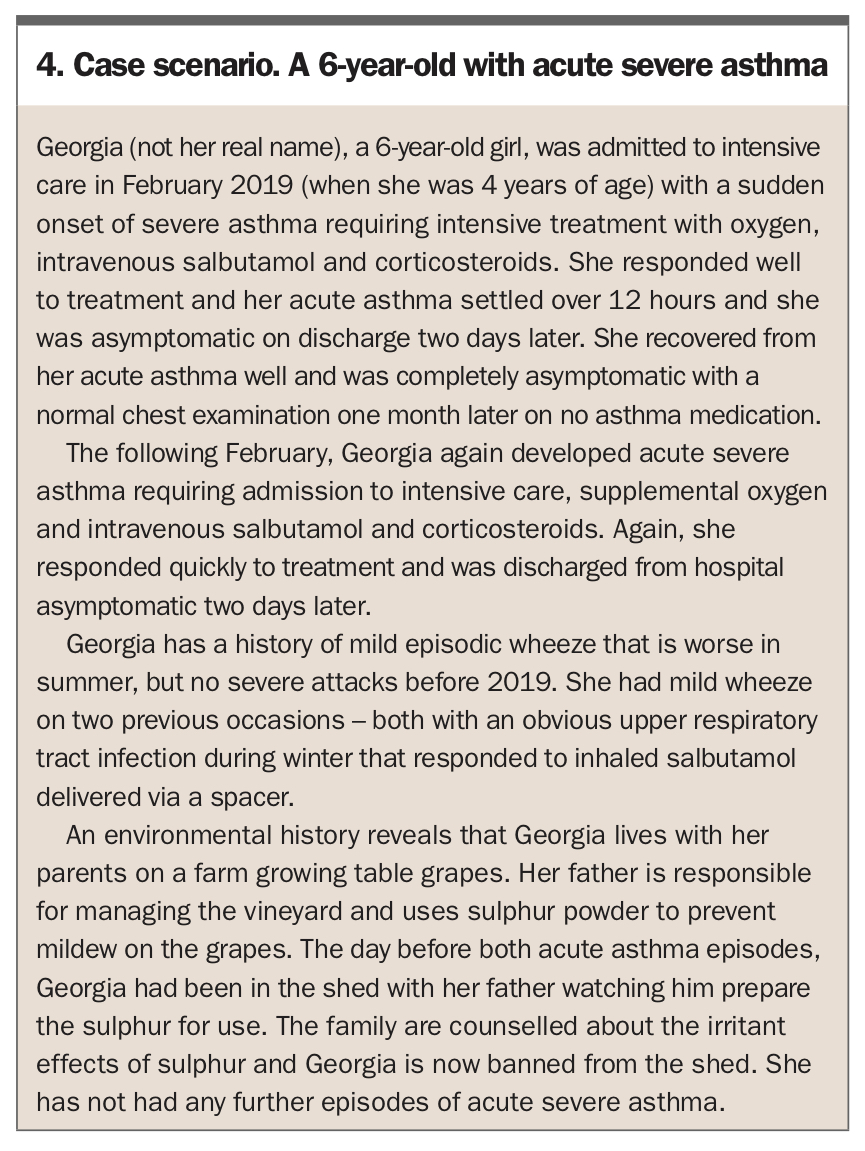
Although most children presenting with respiratory illnesses may not have a significant environmental contribution to the illness causation, an awareness of when to be on alert is helpful. Box 3 outlines circumstances in which doctors caring for children should consider an environmental contribution to the presentation and take an environmental exposure history. A real-life case scenario of a child with sudden onset of severe asthma is presented in Box 4.
{kind=link}
{kind=link}
Conclusion
Although the management of respiratory conditions in children is usually straightforward, when first-line management is not working clinicians should question whether adverse environmental exposures may be playing a role. Taking an environmental history is simple and should not add much time to a consultation. However, the pay-off may be large. When children with asthma are exposed to sources of pollution that the family can not reduce, such as ambient air pollution, adherence to preventive treatment regimens becomes even more important for maintaining good respiratory health. RMT
COMPETING INTERESTS: None.