Smoking cessation – helping patients quit

Smoking and youth
The extensive health benefits of smoking cessation are undeniable; however, for many patients the concept of quitting can be daunting and difficult. An individualised combination of behavioural support and pharmacological interventions can help support patients to quit smoking.
- Smoking continues to be prevalent in our society and the use of e-cigarettes is increasing.
- Smoking is associated with detrimental health effects, including a higher risk of hospitalisation and death with COVID-19.
- Behavioural support along with treatment of nicotine dependence is the most effective approach to supporting smoking cessation.
- First-line pharmacotherapy options are nicotine replacement therapy, varenicline and bupropion.
- Nicotine e-cigarettes may assist some smokers to quit but there is a lack of evidence regarding efficacy and safety.
Australia has a strong history of public health measures to control tobacco use, including bans on advertising and smoking in public places and mandatory plain packaging. Cessation has also received support through the listing of some smoking cessation pharmacotherapies on the Pharmaceutical Benefits Scheme (PBS). The most recent (2019) prevalence data shows that daily smoking has decreased to 11% of people aged over 16 years, with fewer people aged in their 20s and 30s smoking, but little change in older age groups.1 Daily smoking by Aboriginal and Torres Strait Islander peoples has decreased to 27%, but this is still much higher, particularly among First Nations pregnant women, than in non-Indigenous Australians (10.8%).1,2
Although the use of combustible tobacco has decreased, the use of nicotine in other forms is increasing, particularly in young people. From 2019 data, 4.5% of Australians aged 15 to 24 years are current e-cigarette users, which is about double the prevalence of only three years earlier.1 There is evidence that use of nicotine e-cigarettes by nonsmokers is associated with a tripling of the risk of initiating combustible tobacco use and becoming a cigarette smoker.3
After initial uncertainty, it has become evident that smoking is associated with a higher risk of coronavirus disease 2019 (COVID-19) requiring hospital admission and COVID-related death.4 The COVID-19 pandemic has motivated some people to consider stopping smoking but has also made it more difficult to provide face-to-face smoking cessation services.5
Behavioural support
The most effective approach to supporting smoking cessation is to provide behavioural support for quitting, along with treating nicotine dependence.6 As summarised below, the ‘5As’ (Ask, Assess, Advise, Assist and Arrange) is a comprehensive approach to providing support.
- Ask about and document the smoking status of all patients.
- Assess nicotine dependence, and assess and address barriers to quitting.
- Advise all patients who smoke to quit in a way that is clear but not confrontational.
- Assist patients to quit smoking; agree on a quit plan and recommend pharmacotherapy if nicotine dependent. If the patient is not willing to quit, use a motivational approach, explore barriers and review at future visits.
- Arrange follow-up contact for patients making a quit attempt, starting within a week of the quit day. At these visits congratulate and encourage, review progress and problems, encourage continuation of pharmacotherapy and monitor and manage any medication side effects.
When time is short, as it often is in general practice consultations, the three-step ‘Ask, Advise, Help’ structure, developed by Quit Victoria (https://www.quitcentre.org.au/clinical-tools), can be used (Figure). In this approach, behavioural support can be provided by a service outside the general practice, such as the Quitline (13 QUIT [13 7848]). Quitline services vary across states and territories but most provide a proactive service where a Quitline counsellor will telephone the smoker leading up to and following their nominated quit day. Feedback will also be sent to the referring health professional. The Australian Professional Society for Alcohol and other Drugs (APSAD) has an accreditation process for Tobacco Treatment Specialists, who come from a range of discipline backgrounds. GPs can contact APSAD via its website (www.apsad.org.au) to see if there is a Tobacco Treatment Specialist in their area.
Nicotine dependence
Professor Michael Russell, a British tobacco researcher and one of the early proponents of nicotine replacement therapy (NRT), famously said, ‘People smoke for nicotine, but they die from the tar’. Although he may have underestimated the harmful effects of nicotine, the message that nicotine is a key driver of tobacco addiction remains as true as ever. Of people who smoke, about 70% will become nicotine dependent and the propensity to do so is largely genetically determined. The time to the first cigarette of the day is a quick and accurate way of assessing nicotine dependence: if the person smokes within half an hour of waking then it is reasonable to consider them nicotine dependent and likely to experience withdrawal effects (such as irritability and difficulty concentrating) on cessation.
Pharmacotherapy for smoking cessation
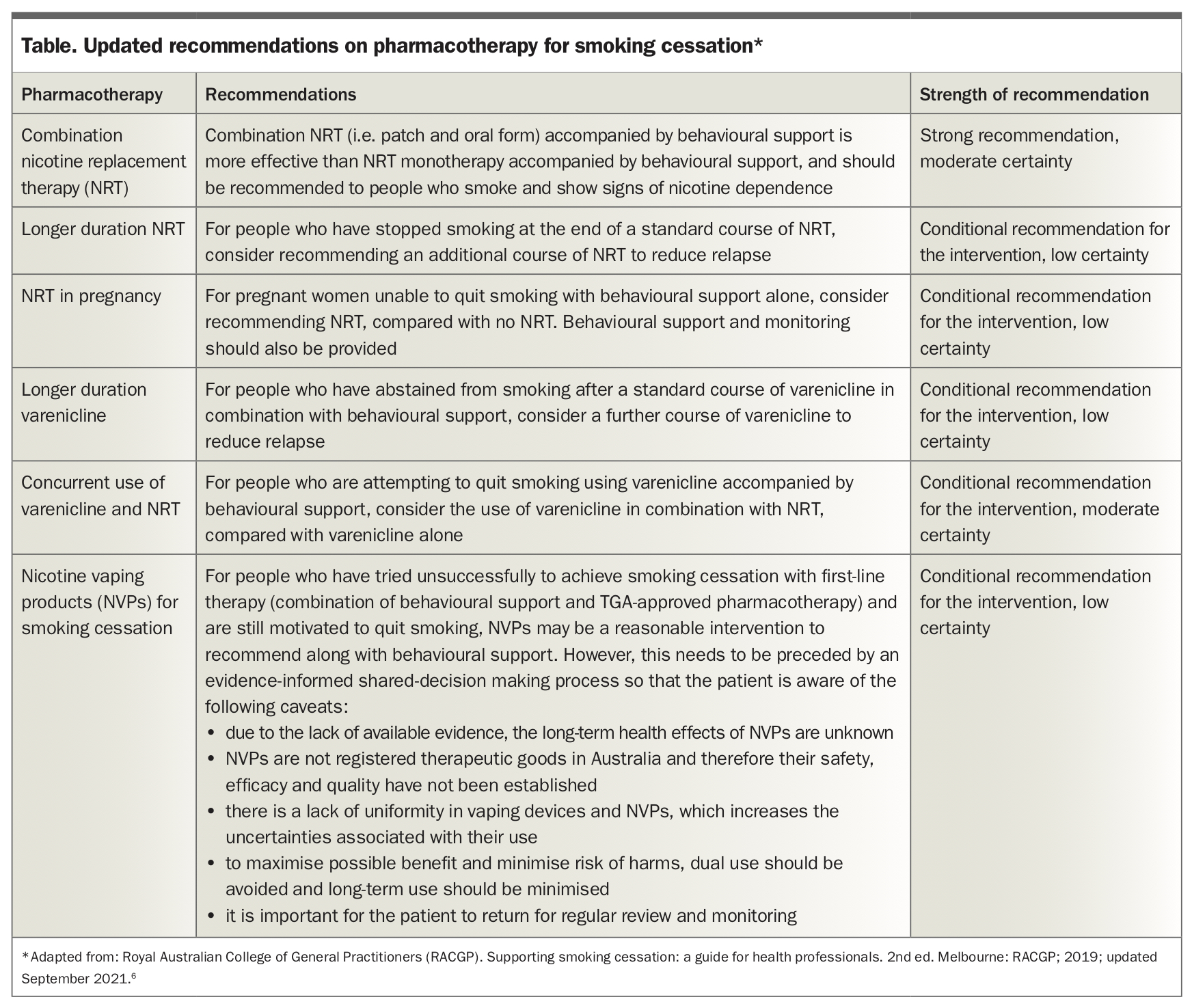
First-line pharmacotherapy options are medicines that have been shown to be effective in, and are registered for use for, smoking cessation. In Australia, the current first-line options are NRT, varenicline and bupropion sustained-release. Based on evidence from a Cochrane network analysis of randomised trials, the most effective medications are combination NRT (a patch plus a rapidly acting oral form) and varenicline, and either of these is therefore the preferred option for most patients.6,7 Bupropion is less effective and recommended for use where the patient is not suitable for NRT or varenicline. For the best effect, pharmacotherapy should always be provided together with behavioural support.6 Recommendations on key questions related to pharmacotherapy are shown in the Table. These updated recommendations are based on systematic reviews carried out for the RACGP by the Joanna Briggs Institute.6
{kind=link}
Quality use of smoking cessation medicines
Lack of uptake and poor adherence to smoking cessation pharmacotherapy are common and have a negative effect on quitting success. It is estimated that up to 20% of people prescribed a smoking cessation medicine never fill the prescription.8 Other common issues are not completing the suggested duration of treatment and/or suboptimal dosing. Ambivalence about using a medicine is a common barrier. Encouraging adherence is important, and one approach is to use the metaphor of a cast for a broken bone. As with a healing fracture, it takes time (typically eight to 12 weeks) for nicotine dependence to fade and for the person to start to think of themselves as a nonsmoker. Like a cast, pharmacotherapy provides support over this period.
Nicotine replacement therapy
NRT in various forms (patch, gum, lozenge, mouth spray, inhaler) has been available for a substantial period of time, both on prescription and over the counter. When used as monotherapy, all forms of NRT are similarly effective (increasing six- to 12-month quit rates by about 6% compared with placebo).6
There is evidence that combination NRT (using a patch with a rapidly acting oral form) is more effective than monotherapy (increasing six- to 12-month quit rates by 5% compared with NRT monotherapy), without any increase in adverse effects.6 It is, therefore, the preferred option; however, only monotherapy is currently subsidised on the PBS. A typical combination NRT dosing regimen is a patch plus an oral form such as 2 mg gum, 2 mg or 1.5 mg lozenge, 1 mg mouth spray or 15 mg inhaler. The oral form may be needed every one to two hours, depending on the person’s experience of cravings or cues to smoking.
Pre-cessation treatment with nicotine patches (two weeks before ‘quit day’) can improve success rates, and is both approved by the TGA and subsidised on the PBS. Once ‘quit day’ is reached, the patch is continued and oral forms can be added as described above (combination NRT). Longer-term treatment (e.g. an additional eight weeks) to help reduce relapse can be considered in those who are abstinent at the end of a standard course of treatment. However, only a maximum of 12 weeks of therapy is subsidised by the PBS in each 12-month period.
The effectiveness of NRT as an over-the-counter consumer medicine has been low, emphasising the need to provide behavioural support as well as pharmacotherapy.
There continues to be uncertainly about the effectiveness and safety of NRT in pregnancy.6 Nonpharmacological options to support quitting should be offered to women who are pregnant or those planning a pregnancy. If these are not successful, the clinician might suggest NRT after an evidence-informed discussion about benefits and risks. Behavioural support and follow up should be provided.
Varenicline
Varenicline is a nicotinic receptor partial agonist and acts to relieve nicotine withdrawal symptoms as well as reducing the reward effect of smoking. Like combination NRT, varenicline more than doubles the rate of quitting at six months follow up compared with placebo. Unlike bupropion, it has few drug interactions. Evidence from a small number of randomised trials suggests that varenicline coadministered with a NRT patch can be more effective than varenicline alone (relative effect 1.62, 95% confidence interval [CI], 1.18 to 2.23).6 As with NRT, there is evidence that a longer course of treatment may reduce relapse in people who have managed to quit after a standard 12-week course. The PBS will subsidise up to 24 weeks of continuous treatment in each 12-month period. A common side effect, seen in 30% of users, is nausea, which is lessened by gradual dose titration and taking the medicine with food.6
Neuropsychiatric adverse effects and the question of whether varenicline can be used safely in people with a history of severe mental illness have been the subject of considerable research. Meta-analyses of randomised trials and observational studies have not supported a causal link between varenicline and these symptoms. Smoking cessation itself can be associated with short-term neuropsychiatric symptoms, such as mood changes and sleep disturbance; all patients should be encouraged to seek assistance if these symptoms are causing distress.
At the time of writing, availability of varenicline is a major problem following a recall of Champix because of concerns about potential contamination of varenicline medicines with the nitrosamine impurity, N-nitrosovarenicline. The TGA website states that this product will not become available again until the end of October 2023. In response to the global shortage of varenicline, the TGA have approved the import and supply of APO-Varenicline 1 mg tablets from Canada under section 19A of the Therapeutic Goods Act 1989. APO-Varenicline is not registered on the Australian Register of Therapeutic Goods, nor is it listed on the PBS. Questions about supply can be directed to Apotex Pty Ltd on 1800 276 839. If there is difficulty obtaining access to varenicline, it is important to explore whether the patient has had an adequate trial of NRT. Many patients have used over-the-counter NRT but have not tried combination NRT and have not done this accompanied by behavioural support from their GP or the Quitline. Bupropion (see below) is another TGA-approved option.
Bupropion
Sustained release bupropion, available on the PBS for nicotine dependence, is similar in effectiveness to NRT monotherapy and has been tested in a variety of populations, including people with depression, cardiac disease and respiratory disease. Due to risk of seizures, it is contraindicated in people with a history of seizures, eating disorders and those recently treated with monoamine oxidase inhibitors. Seizure risk is increased if bupropion is taken at the same time as selective serotonin reuptake inhibitors or tricyclic antidepressants. Adverse effects include sleep disturbance, headache, dry mouth and nausea. Due to its lower effectiveness, interactions and adverse effects, bupropion sustained-release is principally used for patients who are not suitable for combination NRT or varenicline.
Second-line pharmacotherapy options
Given the modest effectiveness of smoking cessation medicines, some patients will not manage to quit despite an adequate trial of one of the first-line options. In such instances, the GP and patient might consider use of a second-line option. These products and medicines are not approved by the TGA for the purpose of smoking cessation.
Nicotine e-cigarettes
Nicotine e-cigarettes are electronic devices that deliver a vapour containing nicotine and other substances, such as glycerol, propylene glycol and molecules from flavouring agents. To date, no nicotine e-cigarette has been through any country’s medicine approval process, and in some countries (such as the USA, UK, Canada and New Zealand) nicotine e-cigarettes are available as a consumer product. Australia has taken a unique approach: from 1st October 2021, under the Therapeutic Goods (Standard for Nicotine Vaping Products) (TGO 110) Order 2021, nicotine vaping products (NVPs) can only be legally obtained, either domestically or imported from overseas, if the user has a valid Australian medical prescription. The aim of this change in regulation was to make nicotine e-cigarettes available to support smoking cessation while reducing access to these products by nonsmokers, particularly young people. The term ‘NVP’ describes products that contain nicotine (in salt or base form) in a solution designed to be inhaled using a vaping device. This includes vape liquids, e-liquids and e-juices that contain nicotine, and the nicotine solution in nicotine e-cigarettes and pods.
There remains a lack of high-quality evidence on the effectiveness of nicotine e-cigarettes for smoking cessation. A review conducted by the Australian National University to inform the RACGP Smoking Cessation Guidelines found only two randomised trials meeting inclusion criteria (with a total of 1468 participants) that compared nicotine e-cigarettes (nicotine concentration greater than 0.01 mg/mL) with nicotine replacement therapy. The relative effect was 1.67 (95% CI, 1.21 to 2.28).9 The RACGP Expert Advisory Group concluded that nicotine e-cigarettes are associated with a small benefit in smoking cessation in the clinical setting compared with NRT, although the certainty of the evidence is low.6 The conclusion and recommendations reached by the Expert Advisory Group and published in the September 2021 RACGP smoking cessation guidelines, along with pharmacotherapy recommendations that were new in the 2019 version, are shown in the Table.6
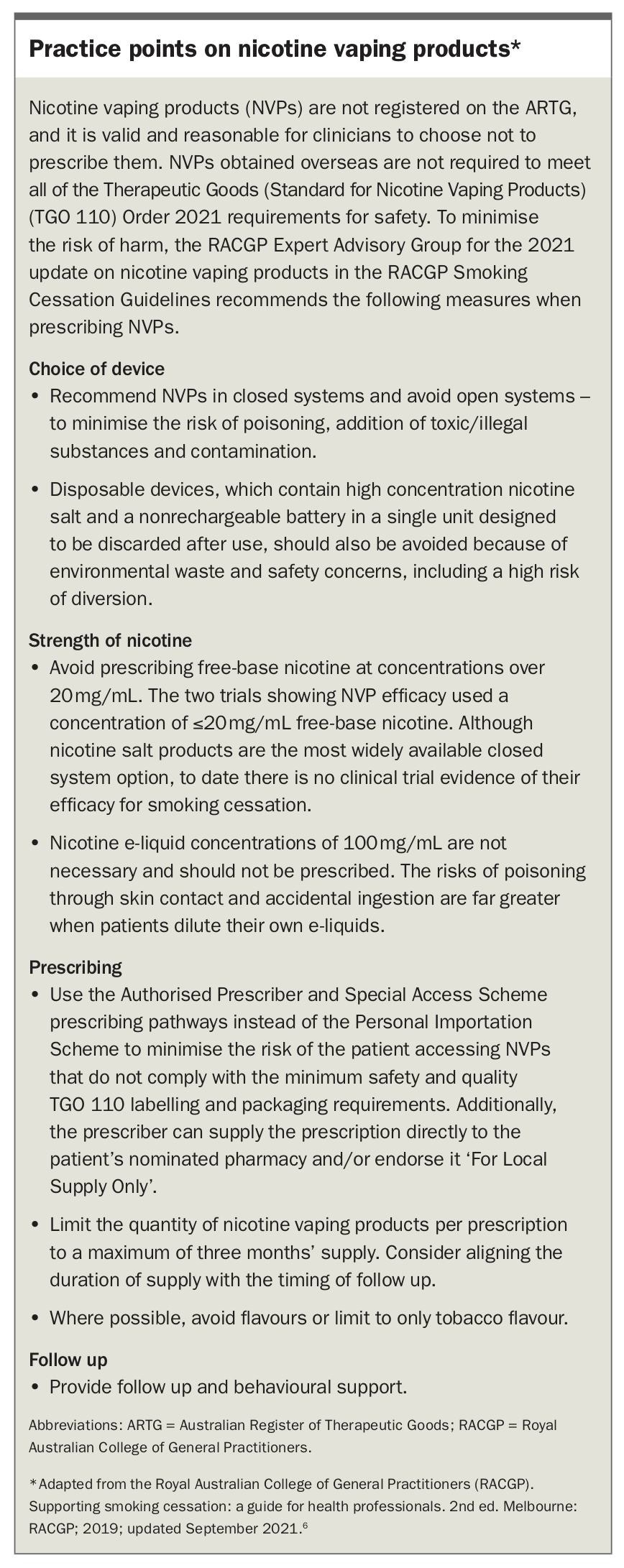
The RACGP guidelines include several recommended practice points to maximise the possible benefits and minimise the risks of prescribing NVPs, as listed in the Box.6
{kind=link}
Nortriptyline
There is evidence from a small number of randomised trials that the tricyclic antidepressant nortriptyline can increase rates of smoking cessation compared with placebo.6 Nortriptyline is limited in its application by its common adverse effects, including dry mouth, constipation, nausea and sedation. There is also a risk of arrhythmia in patients with cardiovascular disease and the medication is dangerous in overdose. The dose and duration for smoking cessation is usually 75 mg for 12 weeks.
Cytisine
Cytisine is an alkaloid extracted from the seeds of the laburnum tree that has been used to support smoking cessation for over 50 years in Eastern and central European and central Asian countries. The mode of action is similar to varenicline, in that cytisine is a selective partial agonist at nicotinic acetylcholine receptors.
There is randomised trial evidence of effectiveness compared with placebo.10 The study showed a higher rate of gastrointestinal adverse effects in the cytisine group compared with the placebo group but the rate of discontinuation of medications was similar between groups. A recent trial conducted in Australia comparing cytisine with varenicline in a noninferiority trial failed to show noninferiority; however, the difference in smoking cessation outcomes was small and the noninferiority threshold was only narrowly crossed.11 The authors noted that the duration of a standard course of treatment may have been a factor (25 days for cytisine compared with 84 days for varenicline). Cytisine is not on the ARTG but some consumers are purchasing the product online.
Smoking cessation in high risk groups
The prevalence of tobacco use is not evenly distributed across the Australian population and some groups have disproportionally higher rates of smoking and harms resulting from tobacco use. As previously mentioned, Aboriginal and Torres Strait Islander people have higher smoking rates and addressing this situation is critical to closing the gap on health outcomes. The Tackling Indigenous Smoking website has a range of resources (https://tacklingsmoking.org.au) and there is a specific Aboriginal Quitline staffed by Aboriginal counsellors.
Another high prevalence group is people with mental health problems. Smoking rates are particularly high among people with schizophrenia, but are also raised in people with depression and anxiety disorders. It is important to recognise that many people with mental health problems are motivated to quit but may need more intensive support and follow up. A positive message is that people who quit report reduced depression, anxiety and stress compared with continuing smokers.
People in prison are a high prevalence group who often have coexisting mental and physical health problems.12 Also, people who identify as homosexual, bisexual, transgender or intersex (LGBTI) have a higher prevalence of smoking; commonly cited reasons (based primarily on US data) include minority stress due to the effects of discrimination, harassment and violence, lack of social support, and fear of weight gain.13
In patients with chronic obstructive pulmonary disease, smoking cessation is the intervention that has the greatest impact on disease progression. Smoking cessation is also vital in the primary and secondary prevention of coronary artery disease. Avoiding smoking in pregnancy and after delivery is vital for the health of both mothers and children.
Conclusion
Supporting smoking cessation is a vital role of general practice and one of the most cost-effective health interventions available. Behavioural support, either in the practice or from a service such as Quitline, can be offered alone or in combination with pharmacological treatment of nicotine dependence. Tested and approved forms of pharmacotherapy are preferred but nicotine e-cigarettes may have a role in a selected group of smokers. Further clinical information, resources and training on smoking and vaping cessation for health professionals are available at the National Quit Training and Resource Centre for Nicotine Cessation website (www.quitcentre.org.au). RMT