Managing asthma in pregnancy

Asthma occurs commonly in pregnancy, and exacerbations are associated with adverse outcomes for the mother and baby. Recent advances in management strategies include the measurement of airway inflammation to guide inhaled corticosteroid treatment.
- Asthma is a highly prevalent medical condition in pregnancy, and exacerbations occur frequently.
- Maternal asthma is associated with an increased risk of adverse perinatal outcomes.
- Active asthma management in pregnancy reduces the risk of some adverse outcomes, including preterm birth.
- Pregnant women with asthma should be treated similarly to other adults with the condition.
- Using the fractional exhaled nitric oxide level to guide treatment is the only intervention shown to reduce exacerbations of asthma in pregnancy, and it may have additional benefits for the baby.
Asthma is the most common chronic disease affecting pregnant women worldwide. In Australia, 12% of pregnant women have asthma.1 Asthma symptoms are variable and unpredictable in pregnancy, and about one-third of pregnant women with asthma experience a worsening of disease.2 Severe exacerbations of asthma occur at a high rate during pregnancy, affecting at least 20% of women.3 Australian studies have shown that between 33% and 45% of women require medical intervention for exacerbations during pregnancy.4,5 These interventions comprise unscheduled GP visits (26% of participants), emergency department presentations (3%), hospital admissions (about 8%) and oral corticosteroid use (15%).4
Association between maternal asthma and outcomes for the child
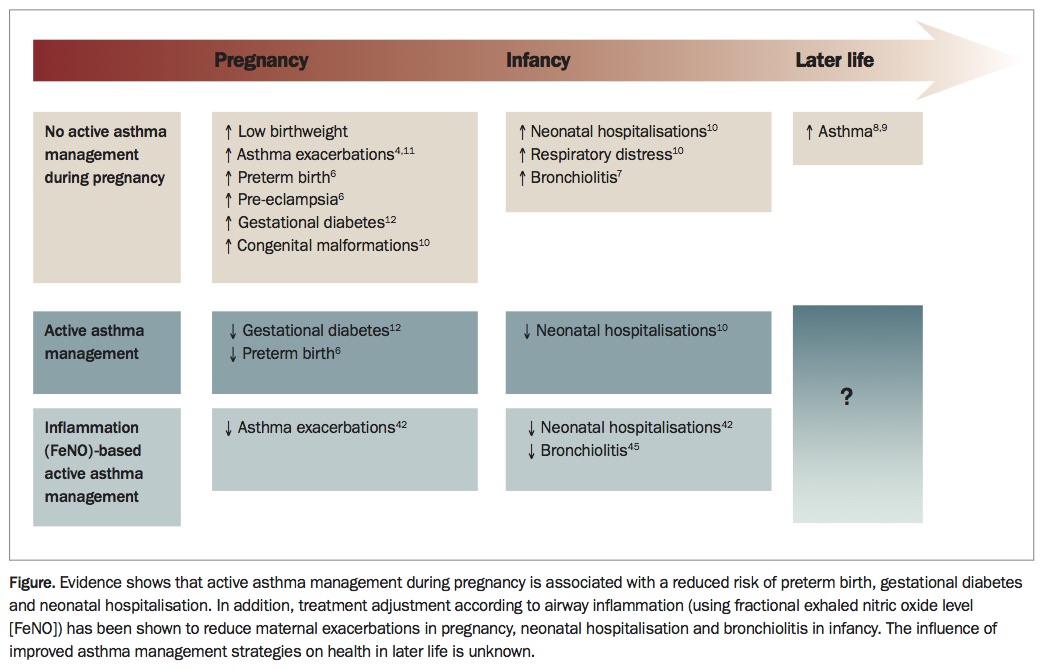
Maternal asthma is associated with risks for the child in the short term (perinatal period, infancy) and long term (childhood) (Figure).6-9 Data from cohort studies conducted between 1975 and 2012 have shown that women with asthma are at increased risk of a range of adverse maternal, placental and neonatal outcomes, with exacerbations further increasing some of these risks.6,10-13
{kind=link}
Reductions in fetal growth associated with maternal asthma have been widely reported. Meta-analysis of 13 studies indicated a 46% increased risk of a low birthweight baby being born to a woman with asthma, compared with babies of women without asthma.6 Further investigation indicated that women who experience asthma exacerbations during pregnancy are three times more likely to have a baby with low birthweight than women who have asthma but no exacerbations.11 Maternal asthma is associated with increased risks of preterm birth, pre-eclampsia, gestational diabetes, caesarean section (particularly elective), perinatal mortality (primarily neonatal death) and neonatal hospitalisation.6,10,12
A small but statistically significant increased risk of congenital malformations has also been reported in babies of pregnant women with asthma (relative risk [RR], 1.11; 95% confidence interval [CI], 1.02 to 1.21).10 This increased risk does not appear to be associated with asthma medications for long-term control, with large studies demonstrating the relative safety of using inhaled corticosteroids (ICS) with regard to congenital malformations.14,15 The mechanisms responsible for these associations remain unclear.
Active asthma management during pregnancy was found to mitigate some of the increased risks described by the meta-analyses. For example, combined data from studies without active management (mostly large retrospective cohorts) have shown a 50% increased risk of preterm birth.6 Conversely, combining data from five studies that provided active management for women with asthma showed the risk of preterm birth was not significant.6 Similar findings were reported with regard to neonatal hospitalisation and gestational diabetes, suggesting that active management may improve perinatal outcomes among women with asthma and their babies (Figure).10,12
Guidelines for managing asthma during pregnancy
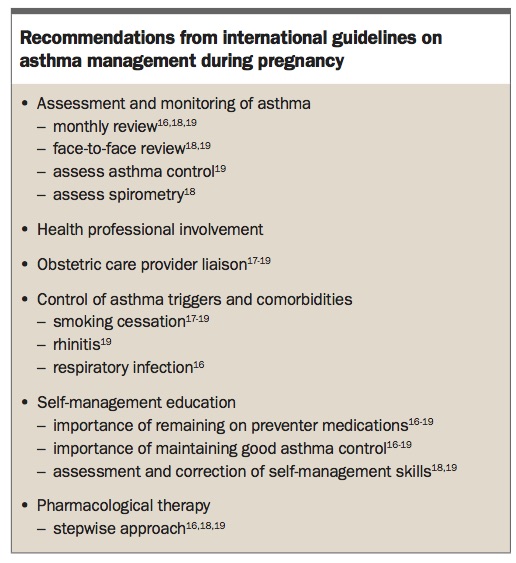
International guidelines on the management of asthma during pregnancy are generally consistent in their main recommendations (Box).16-19 Most recommend monthly monitoring of symptoms, due to the unpredictable course of symptoms in pregnancy. Although the involvement of obstetric care providers and a multidisciplinary team of health professionals is recommended (due to the increased risks of adverse perinatal outcomes), it is unclear whether this occurs in practice. A qualitative study of Australian midwives reported that midwives lacked confidence and were uncertain about their role in asthma management during pregnancy.20 Barriers to their involvement included a lack of knowledge about asthma during pregnancy, lack of time and a lack of referral pathways.21
{kind=link}
Control of asthma triggers and comorbidities is recommended during pregnancy, consistent with recommendations for nonpregnant adults. Comorbidities that are prevalent or problematic in pregnancy include rhinitis, reflux, obesity, depression and anxiety and viral infection.22-24,25 An Australian study found that rhinitis affected 65% of pregnant women with asthma, which was associated with worse asthma control.22 Additional factors that may complicate the management of asthma include smoking and medication nonadherence.5,26,27 Influenza vaccination is recommended for all pregnant women.28 Asthma self-management education is also recommended, but evidence for improvements in skills and knowledge after pregnant women are educated about asthma is limited.26,29
A stepwise approach to pharmacological therapy is recommended during pregnancy, as for other adults.16,18,19 This and other asthma management recommendations for pregnant women are largely based on expert opinion and evidence gathered in nonpregnant adults with asthma, as few randomised controlled trials (RCTs) specific to pregnancy have been conducted.
Budesonide for inhalation (or as a nasal spray for rhinitis) is classified as a category A medication under the Australian categorisation system for prescribing medicines in pregnancy because there is sufficient evidence for its safety from large cohort studies. Evidence for the safety of other ICSs in pregnancy is lacking. One RCT compared budesonide to placebo in a subgroup of women who coincidentally were pregnant while participating in a much larger trial. Pregnancy outcomes revealed no harmful effects of budesonide versus placebo. No data on exacerbations were presented.30 Some guidelines caution against the step-down of ICS therapy in pregnancy, because of the risk of exacerbation; however, there is no evidence that this is harmful or associated with an increased exacerbation risk.16,18,19 For about one-third of women, asthma symptoms may improve in pregnancy.2
Guidelines recommend that patients with asthma exacerbations during pregnancy should be treated similarly to other adults, being given oral corticosteroids (OCS) when indicated and immediate attention if they present to the emergency department (ED) so that risks to the mother and baby are minimised.19 These recommendations are based on clinical experience and expert opinion.19 It is difficult to assess the risks of asthma exacerbations apart from the risks of the medications used to treat them, or from underlying disease severity. One meta-analysis has shown that, compared with pregnant women with asthma who did not use OCS, use of OCS was associated with significantly increased risk for low birthweight (RR, 1.41; 95% CI, 1.04 to 1.93); however, this risk was lower than that for exacerbations (RR, 3.02; 95% CI, 1.87 to 4.89).11
A study in the US described treatment disparities between pregnant and nonpregnant women presenting to the ED. Pregnant women were less likely to be prescribed OCS in the ED or on discharge from hospital.31 This was associated with a higher proportion of pregnant women re-presenting with asthma exacerbations within two weeks.31 This aspect of management has improved in recent years;however, further studies are needed to show whether such differences in treatment derive from women’s or physicians’ attitudes towards medication use during pregnancy.32
New approaches
Recent Australian RCTs in small samples (fewer than 75 women) have shown that pharmacist-led multidisciplinary management and home monitoring of lung function and symptoms with feedback from a health professional can improve asthma control over six months.33,34 However, improvements did not occur in the first three months of the intervention, which is the peak period for exacerbation risk (mid second trimester4,35).
A 2014 Cochrane review summarised the results of eight trials of interventions to manage asthma during pregnancy.36 These trials included 1181 pregnant women with asthma, and only two trials had low risk of bias. Three of the trials tested nonstandard treatments for women experiencing exacerbations;37-39 and the other trials tested pharmacological or nonpharmacological interventions during pregnancy.30,33,40-42 The trial that compared inhaled beclomethasone to oral theophylline for maintenance treatment did not show a difference in exacerbation frequency, and three trials did not report on exacerbations in pregnancy.30,33,40,41
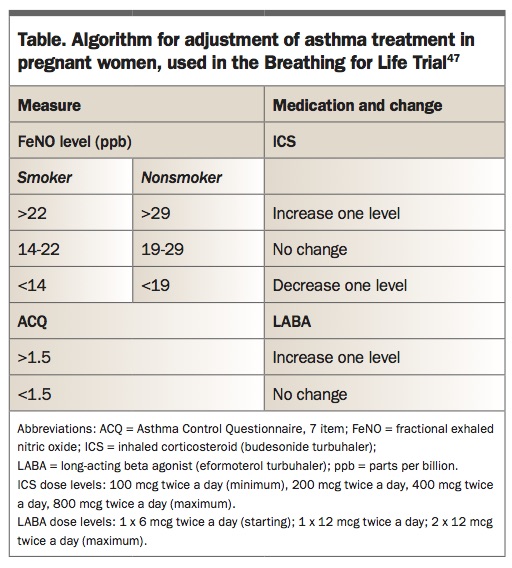
The Managing Asthma in Pregnancy (MAP) study is the only RCT so far to show a significant reduction in the rate of asthma exacerbations during pregnancy.42 This trial compared two management strategies for adjusting ICS treatment from the second trimester of pregnancy to birth. In the control group, maintenance therapy was adjusted based on symptoms, using the Asthma Control Questionnaire to determine the level of asthma control. In patients with uncontrolled asthma, treatment was increased by one step. If asthma was well controlled, treatment was decreased by one step, and no changes were made to medication if asthma was partly controlled.43,44 In the intervention group, medications were adjusted based on the fractional exhaled nitric oxide (FeNO) level, which is a measure of eosinophilic airway inflammation, and on symptoms (Table). When the FeNO level exceeded the upper cut-point (29 parts per billion [ppb]), ICS dose was increased in a stepwise manner to a maximum of 1600 mcg/day, and when it was below the lower cut-point (19 ppb), ICS dose was decreased by one step. In the mid-range (FeNO, 19 to 29 ppb) no change in ICS dose was made. However, when the FeNO level was 29 ppb or less, long-acting beta agonists (LABA) could be added if symptoms remained uncontrolled.42 Cut-points for smokers and nonsmokers were derived from a pilot study of pregnant women with asthma, with the lower cut-point representing the upper 95% confidence limit for stable controlled asthma and the upper cut-point representing the lower 95% confidence limit for uncontrolled eosinophilic asthma.
{kind=link}
Use of the FeNO level to guide treatment achieved a significant 50% reduction in the rate of asthma exacerbations in pregnancy, with a number needed to treat of six.42 This management strategy led to significant variation in the treatment profile compared with treatment guided by symptoms alone. It increased the likelihood of the women being prescribed an ICS or ICS/LABA combination therapy and lowered the mean dose when an ICS was prescribed.42 Combined ICS/LABA medicines are rated pregnancy safety category B3; there are fewer studies on their safety in pregnancy than for ICS alone.19
Outcomes for infants
As yet, no intervention in pregnancy has been confirmed to improve perinatal outcomes for infants of mothers with asthma. In the MAP study, infant follow up in the first year of life found the FeNO-based strategy was associated with a significant reduction in recurrent episodes of bronchiolitis and croup.45 In addition, follow up at age 4 to 6 years demonstrated a lower prevalence of doctor-diagnosed asthma among those whose mothers were managed with the FeNO-based strategy.46 This suggests there may be longer-term benefits for offspring from optimising asthma management in women during pregnancy, as well as a potential for FeNO-based asthma management in pregnancy to be a primary prevention strategy for children at high risk of developing asthma. The Breathing for Life Trial is testing whether a FeNO-based approach to management improves outcomes for babies at birth (assessed as a composite of preterm birth, intrauterine growth restriction, neonatal hospitalisation and perinatal mortality) and reduces asthma prevalence in childhood.47
A 2017 review on asthma in pregnancy noted a lack of studies on the role of diet and nutritional therapy in women with asthma during pregnancy despite a high occurrence of nutritional problems.48 Nutritional problems include gestational diabetes, poor nutritional status, overweight and obesity and excessive gestational weight gain; all of which increase the risk of poor health outcomes for the child.12,23,49,50 Asthma exacerbations in overweight and obese pregnant women are double that of healthy weight women.23 This is a significant finding because exacerbations further increase the risk of poor perinatal outcomes and childhood asthma.8,11 Further work is needed to identify the benefit of modifying lifestyle factors or coexisting morbidities during pregnancy in women with asthma.
Conclusion
Key requirements for further improving the management of asthma in pregnancy are better evidence as well as management guidelines that reflect the available evidence specific to pregnancy. FeNO-based asthma management during pregnancy has been shown in an RCT to successfully reduce the asthma exacerbation rate and may have long-term positive health consequences for offspring.42,45,46 However, current guidelines do not acknowledge the results of this RCT in their recommendations. Further work is testing the effectiveness of this intervention against usual care, and its efficacy for reducing exacerbations among smokers, as well as exploring the acceptability and feasibility of the intervention for antenatal clinic settings from the perspective of health professionals and mothers with asthma. This work is expected to provide the evidence needed to translate this novel management strategy into clinical practice to improve the health of mothers with asthma and their children.47 RMT