Paediatric asthma: update on the stepwise management approach

Dr Haggie is a Staff Specialist General and Respiratory Paediatrician at Shoalhaven District Memorial Hospital, Nowra; and a Research Fellow in the Department of Respiratory Medicine, The Children’s Hospital at Westmead, Sydney (@stuarthaggie). Dr Robinson is a Senior Staff Specialist and the Lloyd Nuttall Asthma Research Fellow in the Department of Respiratory Medicine, The Children’s Hospital at Westmead, Sydney; a Clinical Associate Professor in the Discipline of Child and Adolescent Health, Children’s Hospital at Westmead Clinical School, Faculty of Medicine and Health, The University of Sydney; and Research Associate in the Airway Physiology and Imaging Group, Woolcock Medical Institute of Research, Sydney, NSW (@DrPLungResearch).
Asthma in children
The 2019 and 2020 updates to the Australian Asthma Handbook (versions 2.0 and 2.1) included a major update to evidence and advice on managing asthma in infants and children. Enhanced adherence to these guidelines is crucial for efforts to address the ongoing concern about preventable asthma deaths in Australia.
- The stepwise approach to management of childhood asthma differs by age group (0 to 12 months, 1 to 5 years, 6 to 11 years and 12 years and over).
- Before any stepwise increase in asthma preventer treatment, clinicians should reconsider the diagnosis of asthma, check the parents’ and child’s understanding of asthma management and treatment adherence, and minimise exposure to triggers and environmental tobacco smoke.
- Asthma should be considered as a chronic remitting and relapsing condition, with any hospital presentation representing evidence of inadequate disease control.
- Asthma exacerbations should be considered as a red flag and prompt review of current management.
- Children should be referred for specialist paediatric assessment if they have:
– continued poor symptom control or airflow limitation on spirometry despite appropriate asthma preventer management
– more than two courses of systemic corticosteroids per year or more than one hospital presentation per year
– limitations on school attendance or participation in activities
– any life-threatening episode of asthma.
In Australia, the prevalence of asthma in children aged 0 to 14 years approaches 10%, with higher rates among Indigenous Australians and those living in lower socioeconomic areas.1 Asthma is the fourth most common paediatric emergency presentation and the sixth most common reason for referral to a paediatrician.2,3 The National Asthma Council Australia publishes treatment guidelines in the Australian Asthma Handbook (AAH), based on evidence, where available, and on expert consensus opinion. The most recent major update released in March 2019 (version 2.0 of the online edition) included a major update to evidence and advice on managing asthma in infants and children. Changes affecting the use of preventer as reliever treatment for adolescents included in the minor upate released in September 2020 are also discussed here.4
Despite widespread availability of national and international asthma management guidelines, clinician adherence to guidelines remains inadequate and inferior to the reported adherence for many other chronic conditions.5 Most clinicians asked about the frequency of rescue inhaler use, but the impact of asthma on normal daily activities and frequency of nocturnal symptoms were less well monitored.6 Provision of a written asthma plan, observation of inhaler technique, use of preventer medication and the approach to ‘difficult-to-control’ asthma have been identified as areas for improvement for primary care clinicians.6,7 Families identify GPs among their most trusted resources for asthma management, reinforcing their important role.8
This article summarises the stepwise approach to asthma management in children recommended in AAH version 2.1 and outlines age-specific aspects that GPs should consider. It updates the review of age-specific management of asthma in children, published in the September 2014 issue of Medicine Today, which was based on AAH version 1.0.9
We also discuss the ongoing concern that asthma deaths, which should be viewed as preventable, continue to occur far too often and that poor asthma control or recent hospitalisation should be recognised as significant risk factors for poor outcomes.10-13 Finally, we describe key aspects of the management of difficult-to-treat asthma at tertiary paediatric institutions to provide context for the medications and approaches GPs may encounter as they support management in primary care.
Treatment guidelines by age
The stepwise treatment approach by age in the AAH categorises children into those aged 0 to 12 months, 1 to 5 years, 6 to 11 years and adolescents, with the last classed together with adults. Within these age groups, pertinent aspects of acute management of wheeze and ongoing maintenance asthma preventer treatment are discussed below. Several statements, although introduced within a particular ordinal age group, have broad relevance across all age groups.
Early childhood wheeze is a highly heterogeneous condition, with several wheeze phenotypes described by important longitudinal cohort studies.14 These wheeze phenotypes are identifiable by the early temporal pattern of wheeze and whether symptoms persist into school age. Although the number of different phenotypes differs across these studies, the Tucson Children’s Respiratory Study descriptions are useful, as transient early wheezers, nonatopic wheezers and IgE-associated wheeze/asthma (‘genuine asthma’).15
In 2008, a European Respiratory Society (ERS) task force described early childhood wheeze (age less than 6 years) in terms of:
- the temporal pattern of symptoms – episodic viral wheeze and multiple-trigger wheeze
- symptom onset or duration of wheeze – transient, persistent and late onset.
There are limitations to these approaches, as some features can be identified only retrospectively, with a lack of strong clinical tools to help identify them prospectively at present.16,17 However, the descriptions contain clues to characteristics that may help identify subgroups during early childhood and their likelihood of responding to particular trials of asthma preventer therapy, as described below.
Children 0 to 12 months
Infants aged 0 to 12 months are considered separately from older children in the 2020 AAH. This change acknowledges the differences in wheeze mechanisms between infants and preschool-aged children and seeks to avoid potential harm due to inappropriate treatment.
Management of acute wheeze in infants
Bronchiolitis is an important cause of acute wheezing, and later wheezing episodes are more likely in children who have been hospitalised with bronchiolitis. Reassuringly, most of these children do not require subsequent hospitalisation. In a longitudinal cohort study of more than 20,000 infants in the UK, 80% of those with relatively severe bronchiolitis (i.e. requiring hospitalisation in the first year of life) did not have further wheezing episodes within the study period, which followed up children to the age of 8 years.18
Recent evidence-based Australasian guidelines on bronchiolitis recommend against routinely trialling short-acting bronchodilator or systemic corticosteroid therapy for infants aged 12 months and younger with bronchiolitis.19 In this group, the predominant aetiology of wheeze is not airway hyperresponsiveness, but relates to small airway calibre, further narrowed by oedema and increased mucus secretion, for which beta2 agonists are ineffective.20 Furthermore, there is good evidence that beta2 agonists are of no benefit (for hospitalisation rate or length of stay) and in fact led to increased adverse events (tachycardia, hypertension, tremor and decreased oxygen saturation) for infants with bronchiolitis compared with placebo.21,22
The findings of a Cochrane review were based on large cohort studies; however, there is likely a small subset of infants who respond to beta2 agonists. The current recommendation from the National Asthma Council Australia is to consult a paediatrician before a therapeutic trial of a bronchodilator or corticosteroid (either inhaled or systemic).4 Identifying which infants should trial bronchodilators remains challenging, and for most infants supportive care (respiratory support and adequate hydration) is all that is required. However, in older infants and those with a history of atopy and a strong family history of asthma, a trial of beta2 agonists may be considered. Important considerations when trialling beta2 agonists are discussed in the older age groups. There is no role for routine corticosteroid therapy in infants with bronchiolitis nor in the subset of infants with a positive response to beta2 agonists.
Asthma preventer therapy in infants
Transient early wheeze is the most common wheeze phenotype in infants. It is generally not distressing for the infant, who thrives despite these symptoms. Cough and difficulty breathing are uncommon, and wheeze may be more prominent with viral illnesses. It is associated with lower initial lung function (which later improves) and is believed to be due to smaller calibre of airways. Therefore, this wheeze does not respond to bronchodilators nor to any other current asthma preventer medication. A three-year randomised placebo-controlled trial treated infants for two weeks following an episode of wheeze of at least three days’ duration. The study reported intermittent ICS had no effect on progression from episodic to persistent wheezing and no short-term benefit during these episodes of wheeze.23
Infants at increased risk of wheeze include:
- those born preterm (especially those with bronchopulmonary dysplasia)
- those with antenatal or environmental exposure to tobacco smoke
- those with previous bronchiolitis caused by respiratory syncytial virus (RSV) or recurrent rhinovirus infections.24
In these infants, viral infections continue to be the most common cause of exacerbations, but other triggers such as environmental tobacco smoke, aeroallergens and air pollution should be considered, and exposure minimised.25
Although the AAH does not give specific recommendations for infants with recurrent or persistent wheeze, insight can be gained from other sources.24 In a recent review, close follow up of infants with recurrent wheeze is recommended, and a trial of inhaled corticosteroid (ICS) with short-acting beta agonist (SABA) therapy as needed may be considered, with a re-evaluation of symptoms after a few weeks. If a good clinical response is observed, a dose reduction or cessation after a few months should be considered. If symptoms recur, continued treatment is indicated.24
Children aged 1 to 5 years
The 2019 AAH moved away from the pattern of symptoms (e.g. infrequent intermittent, frequent intermittent or persistent) to consider clinical severity outcomes to guide preventer management.4 Specific categories are:
- mild (salbutamol as needed at home)
- moderate-severe (requiring systemic corticosteroids and/or emergency department presentation)
- life-threatening (requiring hospitalisation or intensive care).
The recommended preventer medicines in this age group are ICS and montelukast (in children aged 2 years and above).
Wheeze is common in the preschool age group, with nearly one third of preschool-aged children having intermittent wheezing.26 Despite the high morbidity of early childhood wheeze, it is estimated that only 30% of toddlers with recurrent wheeze progress to asthma at age 6 years, and fewer still continue to have wheeze as adults.14
Management of acute wheeze in children 1 to 5 years
Salbutamol can be used on an ‘as-needed’ basis to relieve symptoms during wheezing episodes if a therapeutic trial shows it is beneficial. A child with wheeze who is eating well and playing, without signs of a prolonged expiratory phase or increased respiratory effort, may not require any treatment. When a trial of a bronchodilator is appropriate, the markers of clinical improvement should be considered a priori.
The most useful markers of a response include improvements in oxygen saturation, heart rate and respiratory rate, combined with subjective examination findings such as the child’s level of interaction, ability to speak or vocalise without limitation, use of accessory muscles, pronounced expiratory phase and changes in air entry or wheeze throughout the lung fields. Repeated clinical assessment is essential, and the response, or lack thereof, should be well documented in the clinical record and may indicate an alternative diagnosis.27,28
In the 1 to 5-year age group, viral-induced wheeze does not respond to systemic corticosteroids in the same way as observed in older age groups. Two randomised placebo-controlled trials of oral corticosteroids (OCS) to treat viral-induced wheeze are worth mentioning. A 2009 UK study found no difference in hospital admission rates, whereas a 2018 Perth study reported a relatively modest effect on the duration of hospital stay (less than three hours difference vs placebo).29,30 These differing results may reflect potential inclusion of infants with bronchiolitis in the first study.31 In the acute inpatient setting, OCS use should be reserved for those with a clinical response to bronchodilators and a high clinical suspicion of allergic asthma.32,33
Asthma preventer therapy in children aged 1 to 5 years
Episodic viral-induced wheeze is the most common wheeze presentation, with children having no symptoms between discrete episodes. Multiple-trigger wheeze describes wheeze with additional triggers, such as exercise, allergens, cold air and smoke.25 Multiple-trigger wheeze is more likely to persist into older age groups and is associated with greater impairment of lung function and atopy (asthma, hayfever, eczema or allergies) than viral-induced wheeze.34 However, application of this ERS categorisation in clinical practice can be challenging, as the features may change over time for individual children in the preschool age range.35
As in other age groups, environmental tobacco smoke exposure must be acknowledged to families as an important trigger, and support offered for smoking cessation. A meta-analysis reported the effects of environmental tobacco smoke exposure on asthma morbidity in children aged 0 to 18 years; environmental tobacco smoke was associated with worsening lung function, increased wheeze symptoms and nearly double the rates of hospitalisation for acute asthma compared with children not exposed.36
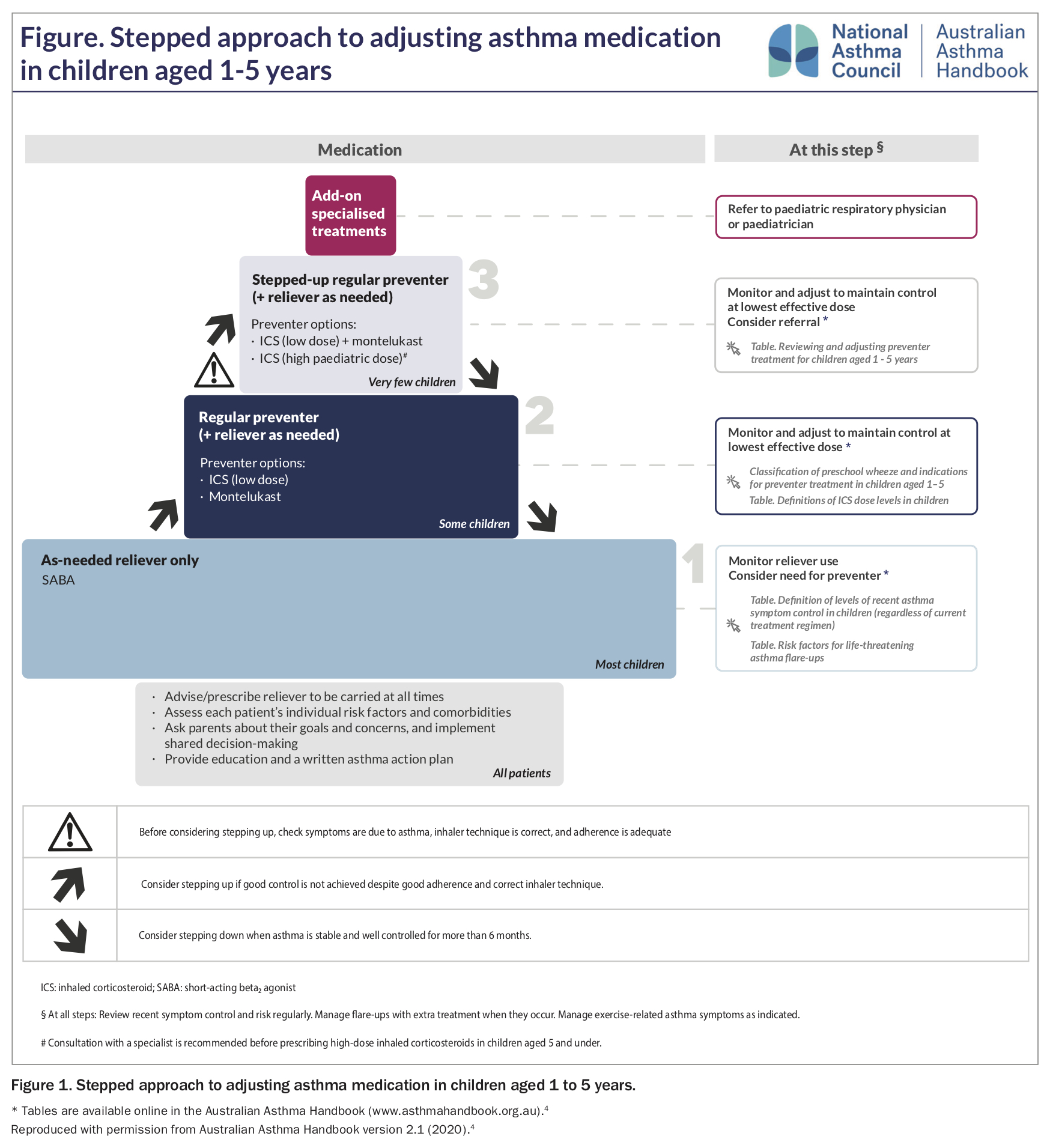
The stepwise approach to maintenance asthma preventer treatments for children aged 1 to 5 years is shown in Figure 1. A trial of preventer therapy is indicated in children with:
{kind=link}
- recurrent episodic symptoms at least once per week or less often if associated with more severe symptoms (OCS treatment or hospital presentation)
- a demonstrated response to bronchodilator therapy, and
- clinical features associated with increased risk of asthma.4
A trial of either an ICS or a leukotriene receptor antagonist (LTRA) may be considered as first-line treatment.37 In preschool-aged children with persistent wheeze, both ICS and LTRA have been shown to reduce SABA and OCS use, as well as the frequency of asthma symptoms.38 The adverse effects of ICS and LTRA are described in the next section but are also applicable to this age group. LABA are not licensed for this age group, and the effects of LABA plus ICS have not been studied systematically in children younger than 4 years.
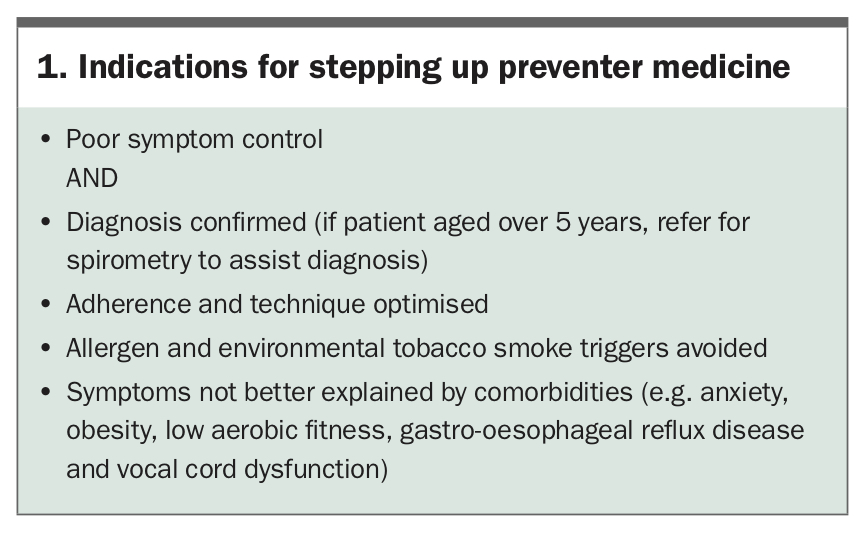
The indications for stepping up preventer therapy are listed in Box 1. Before any increase in preventer therapy, clinicians must:
{kind=link}
- assess patient and family understanding of asthma management and the role of reliever and preventer medicines
- assess adherence to current preventer medicine
- assess spacer technique
- determine whether comorbid obesity, gastro-oesophageal reflux, anxiety or vocal cord dysfunction better account for symptoms
- minimise exposure to asthma triggers and environmental tobacco smoke.
Children aged 6 to 11 years
In children aged 6 years and over, asthma can be diagnosed with certainty, as identifying reversible expiratory airflow limitation using spirometry becomes more feasible, and the incidence of other early childhood wheeze phenotypes has reduced by this age. In children aged 5 years, the feasibility of spirometry is generally above 85%.39
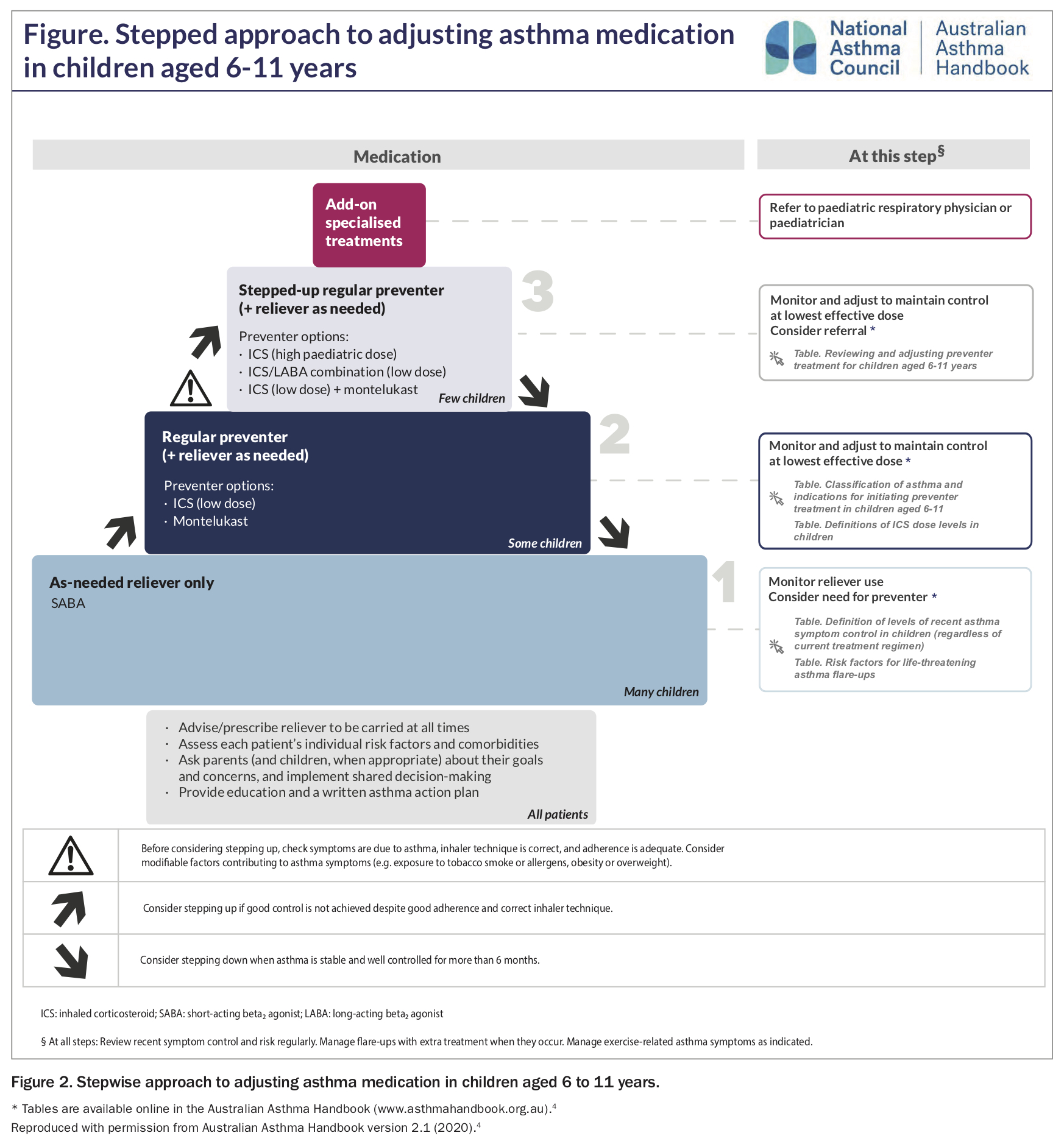
The stepwise approach to maintenance treatments for children aged 6 to 11 years is shown in Figure 2. For children of all ages, the aim of maintenance asthma preventer therapy is to achieve good control of asthma symptoms at the lowest step necessary. Good control of asthma symptoms is considered as:
{kind=link}
- infrequent daytime symptoms (two days a week or less)
- no nocturnal symptoms
- no limitation on play, physical activity or school attendance.4
Before any increase in preventer therapy, clinicians should ensure the diagnosis of asthma is correct, as well as assess family and patient understanding, adherence and comorbidities, and minimise exposure to triggers, as described above for children aged 1 to 5 years.
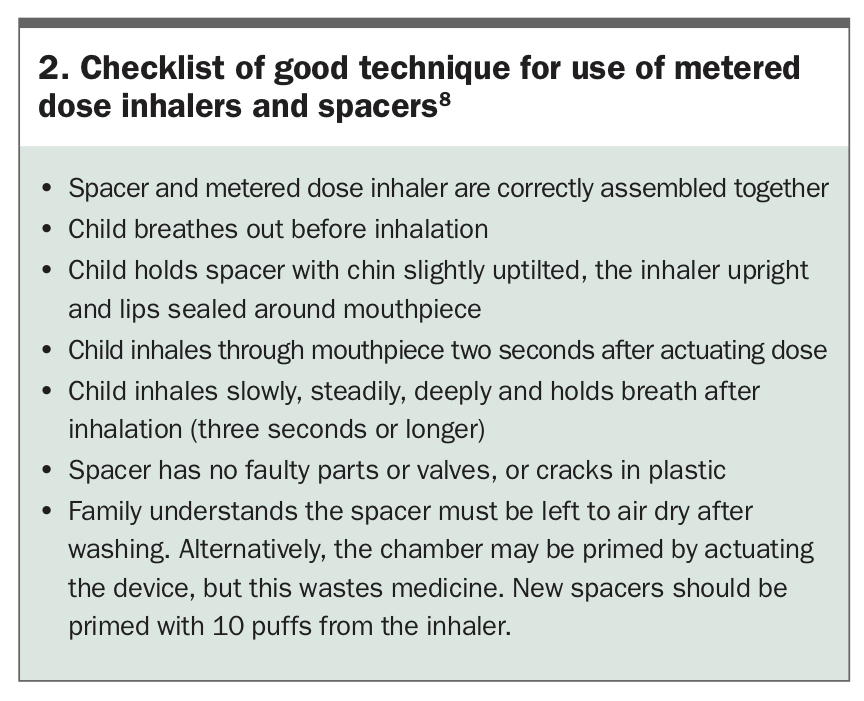
A pressurised metered dose inhaler and spacer is an appropriate first choice for most children.40 Spacers and nebulisers are equally effective means of delivering beta2 agonists to children with acute asthma. However, school-aged children are unlikely to use their devices correctly without careful training and repeated checking of their technique, and parental supervision of medication dosing remains important.41 Asking the child to demonstrate how they use their metered dose inhaler and spacer can offer useful insights into the family’s retention of asthma education and home practices. A useful checklist to detect the most common errors in use of metered dose inhalers and spacers is shown in Box 2.8
{kind=link}
Leukotriene receptor antagonist vs inhaled corticosteroid
An ICS is recommended as the first-line preventer in Step 2 of the asthma management algorithm for children aged 6 to 11 years. This is based on comparative trials favouring ICS over LTRAs for greater efficacy, symptom reduction, exacerbation prevention and lung function improvement.42,43 However, an LTRA may be more effective for some patients, and some may find adherence to LTRAs easier than to ICS.44,45
Inhaled corticosteroids
At higher doses, ICS have been shown to have a relatively flat dose-response curve, with increasing systemic side effects such as adrenal suppression at doses over 400 mcg/day fluticasone propionate equivalent, without increased efficacy.46 A 2004 Cochrane review suggested that commencing an ICS at a moderate dose is as effective as commencing it at a high dose and then reducing the dose while monitoring symptoms.47
Growth suppression due to ICS is dose-dependent, and different age groups differ in their susceptibility to growth effects, with children aged 4 to 10 years being more susceptible than pubertal children.48 A randomised placebo-controlled trial of ICS in children aged 5 to 13 years reported a mean decrease of about 1 cm in height, typically with onset within two years, that was sustained at follow up through to adulthood.49 In children with persistent asthma requiring maintenance ICS treatment to achieve good asthma control, we recommend that this small effect on final adult height should be viewed as an acceptable trade-off for better asthma control.
Leukotriene receptor antagonists
LTRAs are effective for exercise-induced bronchoconstriction, with studies in both adults and children reporting a better response than to other options, including ICS and ICS plus LABA. Patients with exercise-induced bronchoconstriction tend to have a smaller drop in expiratory airflow during exercise and a better response to SABA after exercise when using LTRAs compared with combination ICS plus LABA.50-53
An important aspect to discuss openly with parents from the start of LTRA treatment is the potential for neuropsychiatric adverse drug reactions. These have been of concern and have attracted media attention, and are more common in children than adults. The most common adverse reactions include aggression and sleep disorders in younger children and headaches and depression or anxiety in adolescents.54,55 A retrospective cohort study in children reported the onset of neuropsychiatric adverse drug reactions usually within the first two weeks of commencing an LTRA; treatment cessation was not typically required but led to resolution in those who chose to cease.56 Clinicians should be aware of these associations, discuss them openly with parents and be vigilant for adverse events.
Individual responses to Step 3 treatment
Step 2 treatment with an ICS alone is effective in the vast majority of children with mild persistent asthma.57 In children with poor symptom control despite a low-dose ICS (250 mcg/day fluticasone proprionate equivalent or less), where adherence is considered appropriate, there are several options for treatment escalation. These include a high-dose ICS (500 mcg/day fluticasone proprionate equivalent or more), a combination LABA with low-dose ICS or an ICS plus LTRA.
These three treatment options were compared in a prospective, crossover blinded randomised trial in children aged 6 to 18 years with asthma inadequately controlled by a low-dose ICS (twice daily 100 mcg fluticasone proprionate equivalent).58 Patients were randomly allocated to high-dose ICS (twice daily 250 mcg fluticasone proprionate equivalent), low-dose ICS plus LABA or low-dose ICS plus LTRA in a sequential manner. The study results showed that the optimal treatment differed between individual children. ICS plus LABA therapy was significantly more likely to provide the best response (compared with high-dose ICS or ICS plus LTRA). However, as the composite outcome measure included any improvement in FEV1, and inclusion criteria included a demonstrable FEV1 response to a bronchodilator, the study design may have favoured LABA-containing medications.
These findings highlight the need to consider alternatives in Step 3 of the stepwise management algorithm when asthma control is not achieved despite optimal adherence and education. Other factors such as cost may influence decisions. Currently, LTRA is not PBS-subsidised for patients aged over 15 years, although it may be within financial reach of families as generic montelukast options recently became available.
Adolescents aged 12 to 18 years
The prevalence of asthma declines from about 16% in primary school-aged children to 11% in adolescents.59 As for the management of any chronic illness in adolescence, management of asthma becomes more challenging because of under-recognition of symptoms, erratic self-medication (i.e. decreased adherence), denial of disease severity and risk-taking behaviours.60
Preventing asthma deaths
Asthma mortality in Australia remains higher than in other comparable developed countries such as Canada, France, Japan and Italy.12 Adolescents are over-represented among asthma deaths, comprising up to 60% of cases.12,13
Recent audits of asthma deaths from the UK and Australia, triggered by increasing concern over preventable and escalating mortality, describe children with a pattern of excessive use of reliever medication and underfilled prescriptions for preventer medications, a history of hospital presentations with poor follow-up care, repeated courses of OCS and frequent missed school days.12,13,61,62 Children from vulnerable families are prominent among paediatric asthma deaths, with high rates of family breakdown, parental substance abuse, domestic violence and child protection involvement.12
Damningly, the UK national review of asthma deaths reported that 46% of deaths could have been avoided if patients had been better managed in the year before they died.60 Patients did not receive key areas of routine care, with only 4% managed in line with current national guideline recommendations. Prescribing errors were widespread, acute asthma was poorly managed, and severe cases were not referred to specialist centres.
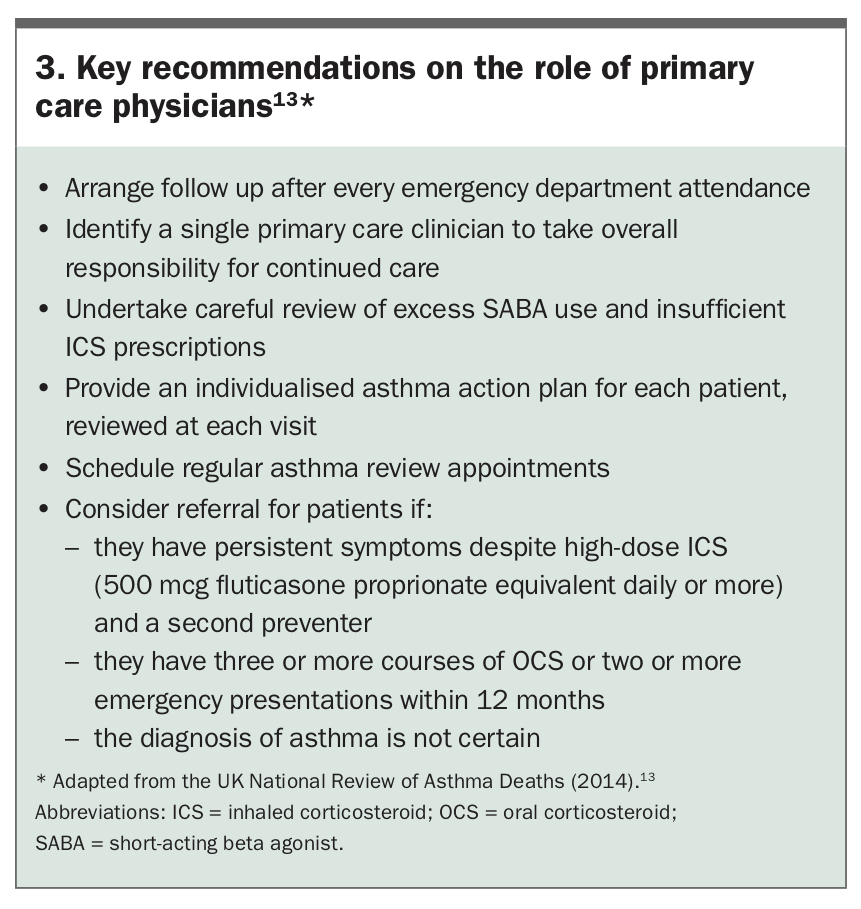
Leading physicians have advocated for a frameshift in the perception of asthma exacerbations, arguing that each acute exacerbation episode should be viewed as a significant marker of poorly controlled disease and prompt a careful review of management.10 Acute asthma attacks carry a risk of further attacks and death. The AAH currently encourages clinicians to increase disease monitoring around these flare-ups and to refer patients with more than one emergency visit in a year or repeated OCS treatments to a specialist centre.4 Recommendations about the key role of primary care physicians from the UK National Review of Asthma Deaths are shown in Box 3.13
{kind=link}
Improving preventer medicine
The underuse of preventer medication and overuse or reliance on SABA treatment has emerged as a key issue in asthma management. This was addressed directly in the latest update of the Global Initiative for Asthma (GINA) committee recommendations, which are considered by the National Asthma Council Australia in developing the Australian asthma guidelines. The 2019 GINA report raised serious concerns about the overuse of SABA reliever treatments paired with the underuse of ICS preventer treatment among adolescents and other age groups.
Specific to the adolescent age range, GINA guidelines recommended that adolescents should receive an ICS whenever a SABA is required, either as a separate ICS inhaler alongside SABA or using combination ICS plus formoterol (a fast-onset LABA). Only patients using SABA once per month need not use an ICS.63 This recommendation is in part derived from large randomised trials mostly in adults, with some adolescent representation, comparing standard treatment with combination ICS plus fast-onset LABA. In these studies the ‘maintenance and reliever therapy’ (MART) approach was shown to reduce rates of severe exacerbations and overall ICS dosing.64-66 The applicability of this recommendation to adolescent management is compromised by the limited representation of adolescents in these studies.
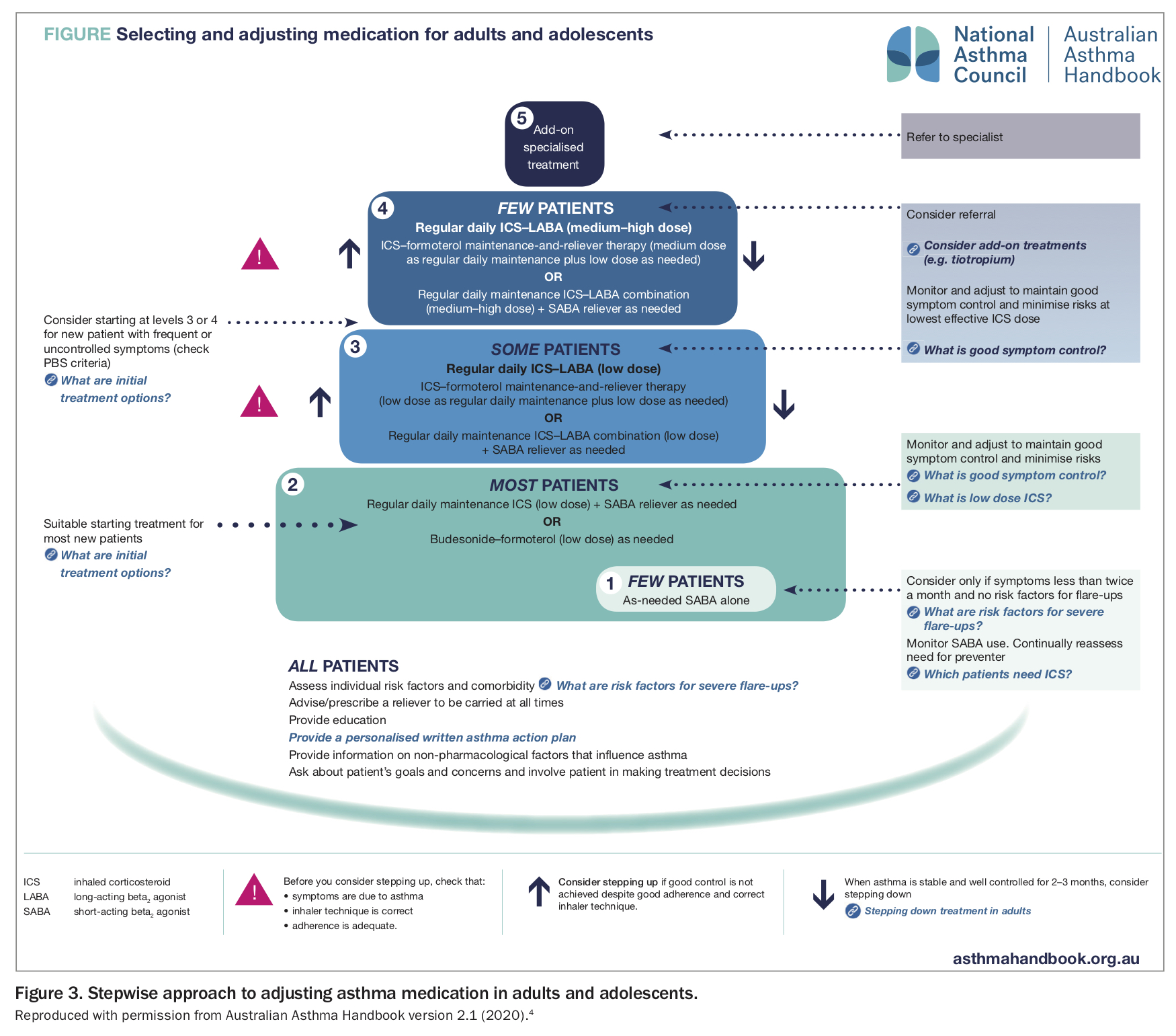
The AAH recently reviewed its recommendations in response to these GINA guidelines and released a minor update in September 2020 (version 2.1). This includes revised recommendations for adolescents (Figure 3).
{kind=link}
The PBS recently added combination budesonide plus formoterol for these indications in anticipation, available in a ‘turbuhaler’ or metered dose inhaler. The inhaler as reliever and treatment approach is considered only for people with mild asthma. Also, only an ICS plus fast-onset LABA combination (budesonide and formoterol) is suitable for this approach; other ICS plus LABA combinations (e.g. salmeterol and vilanterol) are not to be used for this indication.
Other important management aspects across age groups
Stepping down asthma treatment
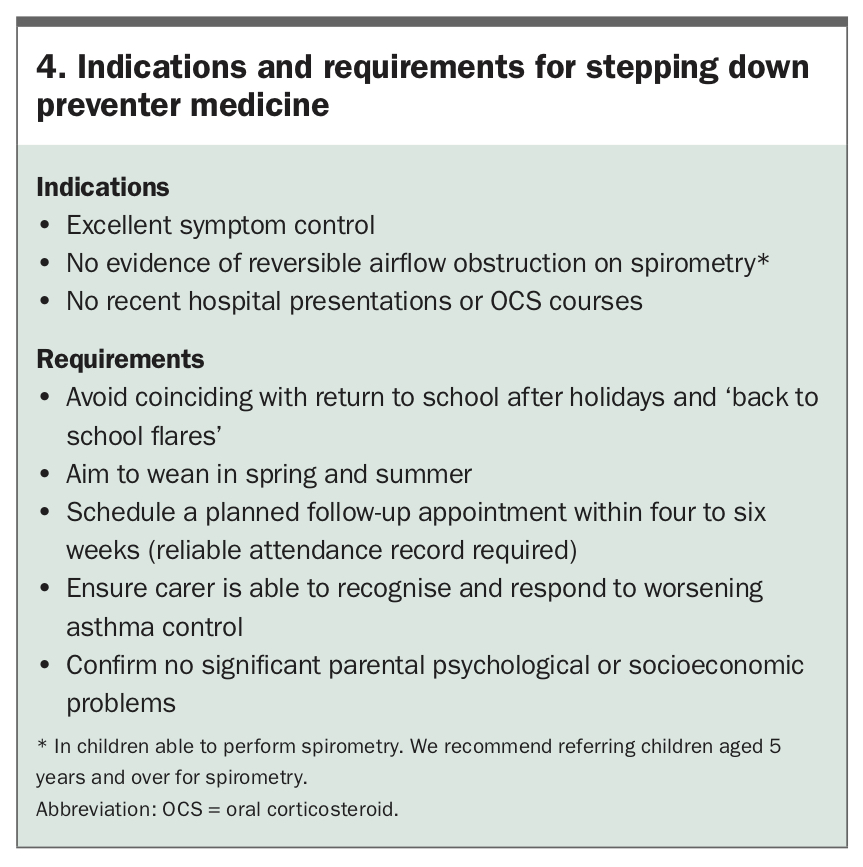
Asthma is considered well controlled when symptoms are absent or mild, occur during the daytime only and quickly respond to a SABA (used less often than twice per week). The patient should have no limitations on play, sport or school attendance, no nocturnal symptoms (AAH) and no recent history of exacerbations managed with OCS or hospitalisation. The indications for step down of asthma preventer medicines are listed in Box 4.
{kind=link}
In patients prescribed ICS plus an additional non-ICS preventer (montelukast, combination ICS with LABA, or a biologic agent), a reduction in ICS dosing while maintaining the other preventer has superior outcomes compared with weaning onto ICS alone. This suggests that tapering ICS dosage by 50% before LABA or LTRA discontinuation may be a preferable approach. Seasonal effects are noted, with greater success in spring and summer than at other times.67 There is a lack of data to guide the rate of reduction, and the lowest dose of ICS needed to control asthma and any reduction needs to consider the individual’s potential for exacerbation, the severity of previous exacerbations and the carer’s ability to manage such an occurrence.
Parent education and asthma plans
The provision of an asthma action plan is not only an important clinical communication between care providers and families but also an important opportunity for focused education. Indeed, research suggests that it is not the asthma plan per se but the education that accompanies it that is associated with better disease control.68 Important aspects for clinicians to address include the pathophysiology of the child’s disease, the use and role of reliever and preventer medicines, expectations of treatment and the threshold for medical review.69 Children provided with education and written action plans have been shown to have significantly fewer asthma exacerbations, OCS prescriptions, loss of school days, nocturnal wakenings and overall symptom scores.68,70
School plans
Schools are importantly placed to support the management of children with asthma. The Asthma Friendly Schools Initiative from North America suggested the development of resources for schools to improve awareness of asthma-related issues and a standardised approach to handling worsening asthma in a child.71 Schools should have an annual process for identifying students with asthma, ensure easy access to inhalers (preferably carry their own), identify and reduce common asthma triggers within the environment and support communication and collaboration between carers, students, educators and healthcare workers.71, 72 Asthma education for school staff increases asthma knowledge and preparedness.73 It is important that teachers receive guidance and training in appropriate asthma care. Schools should also encourage a policy of exercise for all students with asthma.73, 74
Clinicians should be aware of the phenomenon of back-to-school asthma flare-ups; each year, emergency department presentations and hospitalisations surge during the first months of the school year.75 It is important that clinicians recognise the start of the school term as a time to avoid stepping down treatment.4 It is also helpful to plan reviews toward the end of the school holidays, which ensures the opportunity to review and update the asthma action plan and encourage children to communicate their symptoms to teaching staff with the support of their parents.
Medication adherence
Barriers to medication adherence in school-aged children include a lack of motivation, difficulties remembering and social barriers. Children report the paradox that they find parental reminders annoying but that prompting improves adherence.76
It is important to provide practical support to families by openly and compassionately exploring the understanding and obstacles to treatment, and where possible offering strategies to overcome these challenges. Evidence-based strategies to promote adherence include:
- the use of rewards to reinforce adherence
- including treatment within other routines (e.g. mealtime, brushing teeth)
- determining reasonable, specific goals defined by the patient
- using visual or auditory reminders
- using a measure of adherence to benchmark achievement at home
- simplifying treatment regimens (e.g. prescribing once-daily ICS for children aged 12 years and over).76-78
Monitoring devices
Electronic monitoring devices can be fitted to a range of inhalers, and the data downloaded remotely to provide a clear picture of adherence and how it impacts on asthma control and exacerbations. This technology is useful in children with persistent symptoms and difficulties understanding treatment adherence, to avoid unnecessary investigations or overtreatment.79 Currently, these devices are typically used only by tertiary centres for patients with more severe asthma, but pharmaceutical companies are starting to offer them alongside medications to the broader community.
The development of smartphone apps to support adherence is an emerging area. The opportunity exists for digital media to detail symptom scores, medication adherence information and even basic measures of lung function and to communicate these directly to healthcare providers.80 Studies in adults with asthma found that the use of mobile apps improved medication adherence and asthma control.81 The issues with app development include the profit motives of developers that are placed ahead of the health needs of users. In addition, there is an oversupply of low-quality information apps that either are not effective or do not meet patient needs, or that fail to comply with existing evidence-based clinical practice.82
Complex asthma and the role of biologic agents
An estimated 5 to 10% of children with asthma remain symptomatic despite receiving large amounts of asthma preventer treatment.83,84 Children with persisting dyspnoea, chest tightness, wheeze, cough or persistent airflow obstruction on spirometry despite being prescribed Step 4 treatment and are considered as having ‘difficult to treat’ asthma.78,79 This group includes:
- children with poor adherence, who might otherwise have better controlled asthma
- those with comorbid conditions with symptoms that may be mistaken for asthma but do not respond to escalating asthma treatment
- those who do not have asthma but have other diagnoses accounting for symptoms
- those with severe treatment-resistant asthma requiring escalating therapy.80
Although patients with difficult-to-treat asthma represent a small proportion of those with asthma overall, they consume a high proportion of healthcare resources.81
Management of difficult-to-treat asthma
Patients with difficult-to-treat asthma require a systematic approach that:
- confirms the diagnosis and the contribution of asthma to symptoms
- identifies barriers to effective treatments
- manages comorbidities (anxiety, obesity, vocal cord dysfunction, gastro-oesophageal reflux, allergy and rhinosinusitis)
- optimises treatment and monitors for adverse effects.87,88
Within complex asthma clinics, this care is coordinated by a respiratory physician in conjunction with some or all of: an asthma nurse specialist, allergy and immunology physician, respiratory scientist, psychologist, physiotherapist, speech pathologist and ear, nose and throat surgeon.
Severe asthma is considered in patients with a confirmed asthma diagnosis, comorbidities, optimal adherence and a continued need for high-dose ICS plus a second preventer to maintain control or asthma that remains uncontrolled despite this therapy.84 Children with severe asthma have poor quality of life, limitations on activities and frequent asthma attacks and are at high risk of treatment side effects.83
Severe asthma is recognised as a heterogeneous condition, and cohort studies have begun to define phenotypes within this patient group that may allow effective biomarker-driven treatments. Although no specific phenotypes are agreed on, there appears to be a clustering of an early-onset allergic phenotype, a later-onset obese (primarily female) phenotype and a later-onset eosinophilic phenotype. Identifying eosinophilic inflammatory biomarkers is helpful in considering targeted therapy such as biological agents.89,90
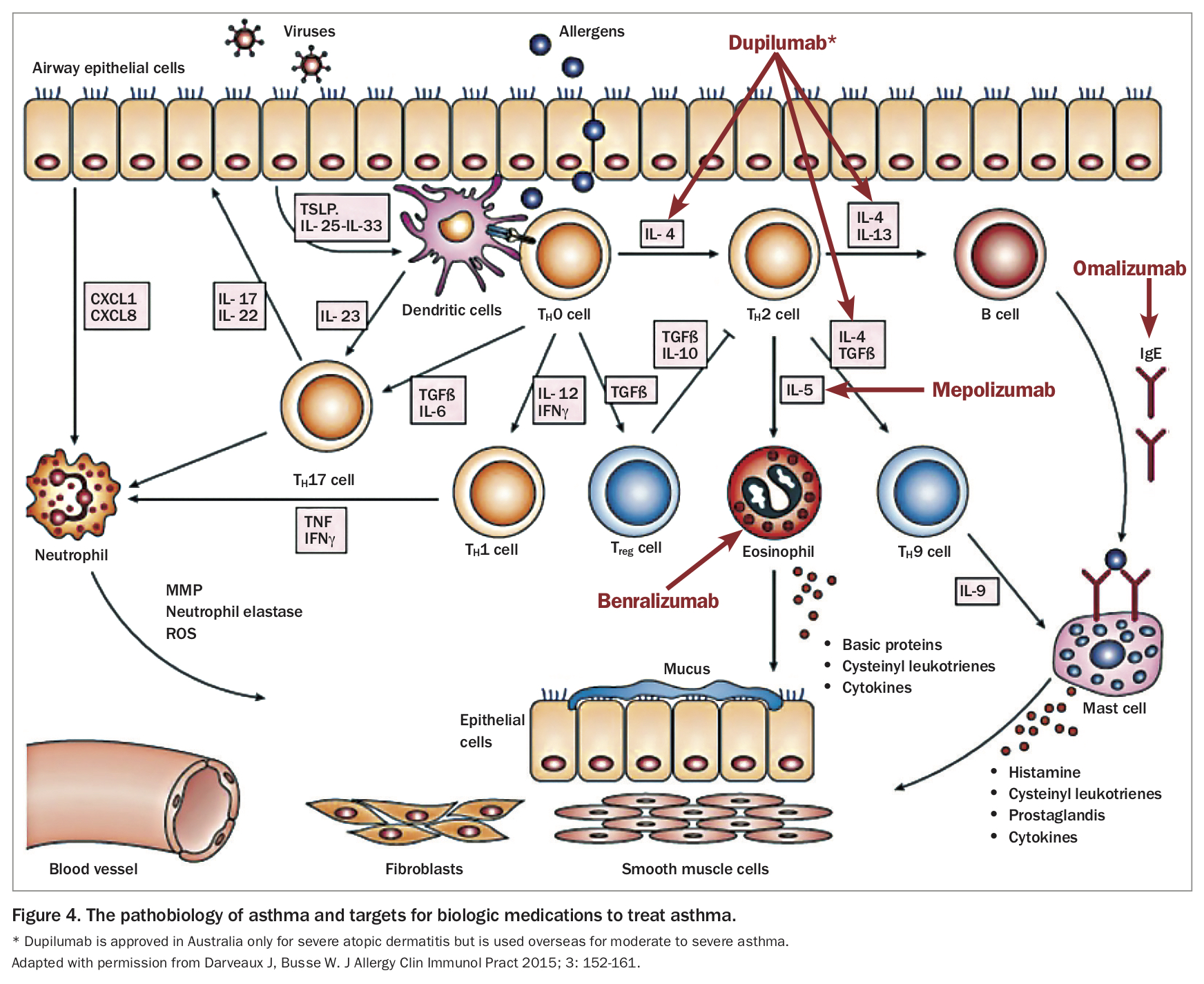
In Australia, three monoclonal antibody treatments are approved for the treatment of severe asthma:
- omalizumab (anti-soluble IgE), which has been used since 2002 for the treatment of severe allergic asthma and was approved for children aged 6 years and over in 2016
- benralizumab (interleukin-5 receptor antagonist), which is available for children aged 12 years and over
- mepolizumab (anti-soluble interleukin-5), which is available for children aged 12 years and over.
The complex inflammatory cascade of asthma and site of action of these agents is shown in Figure 4.
{kind=link}
The use of monoclonal antibodies in the treatment of severe asthma in children has been shown to reduce exacerbations requiring OCS and improve baseline lung function.91-95 These medications are administered by subcutaneous injection, initially every two to four weeks. To be eligible for a PBS subsidy for monoclonal antibody treatment, patients must be known to a respiratory specialist or severe asthma clinic.4 Biologic agents should not be started by primary care physicians; general paediatricians also refer children to a complex asthma clinic for assessment before this step. Once established as an individualised treatment, ongoing follow up and review should continue in a shared care arrangement between the GP and paediatric service.
Conclusion
Management recommendations for paediatric asthma vary by age. However, important principles, such as accurate diagnosis and titration of treatment to maintain adequate control at the lowest preventer medication dose, are applicable to all age groups. Patients with well-controlled asthma should have little need of reliever medication, no limitations on activity and no nocturnal symptoms; this should be the goal for the primary physicians of all patients with asthma. Routine review of patients with well-controlled asthma should focus on revising action plans and reinforcing treatment adherence and drug delivery technique. Patients who have poor day-to-day symptom profiles, require more than one course of OCS per year or are not responding to guideline-recommended treatment must be recognised as a concern and referred for specialist assessment and reviewed more regularly.
Recent asthma mortality reviews have identified important risk factors, such as over-reliance on reliever and underuse of preventer medications. Worryingly, UK research suggests that these patients are not being well identified in primary care. Asthma deaths remain highly preventable, and better recognition of at-risk groups and improved adherence to current management guidelines, such as those outlined in the AAH, is crucial to efforts to reduce asthma mortality. Options to improve adherence are increasing, including once-daily administration options for ICS and ICS plus LABA, asthma-focused apps and electronic monitoring devices. For patients with difficult-to-treat asthma and severe asthma, the armamentarium is expanding with novel biological agents targeted against precise disease pathways. Understanding of how best to identify the phenotypes most likely to respond is improving.
A recent article ‘After asthma – redefining airway disease’ made several thought-provoking recommendations.96 Asthma should be considered an umbrella term, encompassing a collection of distinct airway disease phenotypes alongside comorbidities that may contribute to symptoms. Better appreciation of these components and the developmental trajectories of airway disease will allow clinicians to tailor an individualised approach to asthma management for each patient, trialling and evaluating therapies that have led to a clinical improvement, or not, and considering the treatment of comorbidities that influence disease or influence the perception of symptoms.
Lastly, clinicians must adopt a ‘zero tolerance’ approach toward asthma attacks, recognising them as a red flag, if future efforts to reduce the unacceptable ongoing asthma mortality are to be successful. RMT