Oral corticosteroid stewardship in asthma: an urgent issue

Dr Politis is a Sleep and Respiratory Advanced Trainee at the Monash Lung, Sleep, Allergy and Immunology Department, Monash University Hospital, Melbourne. Professor Bardin is Professor and Director at the Monash Lung, Sleep, Allergy and Immunology Department, Monash University, Melbourne, Vic. Dr Blakey is a Respiratory Consultant at the Respiratory Medicine Department, Sir Charles Gairdner Hospital, Perth; and Adjunct Associate Curtin University Medical School, Perth, WA.
Asthma
Asthma in children
Oral corticosteroid therapy for asthma can be highly effective; however, overuse leads to irreversible harm. Improved asthma control, with reduced need for oral corticosteroid therapy, can be achieved through improved use of common preventative therapy, treatment of comorbidities such as smoking, and early consideration of newer specialist medications.
- Hundreds of thousands of prescriptions for oral corticosteroids (OCS) for asthma are written each year in Australia, often outside the evidence base of their benefit in acute severe asthma.
- A relatively small cumulative exposure carries a significantly increased risk of diverse and serious complications, including sepsis, venous thromboembolism and heart disease.
- Primary prevention of OCS use is achievable for most people through improved diagnosis, appropriate treatment of comorbidities and concordance with preventative therapy.
- Harm reduction is achievable through judicious guideline-based prescribing and dispensing of OCS courses, supported by education.
- Secondary prevention of recurrent prescriptions is achievable and includes early referral to specialist care for multidisciplinary assessment and newer therapies.
Asthma is highly prevalent, affecting about 300 million people worldwide and at least one in 10 Australians.1,2 Despite large advances in treatment, most recently using biological therapies for severe asthma, asthma remains poorly controlled in many patients, who experience regular acute exacerbations. Oral corticosteroid (OCS) treatment can be highly effective for asthma, and widespread prescription remains a feature in Australia and worldwide.3.4 However, this longstanding practice requires consideration given the evidence supporting alternative successful treatments and more recent identification of key dose thresholds for the development of OCS-associated side effects.
In this article, we wish to engage colleagues in respiratory and general practice and prompt you to consider your current practice in this area. We present a brief overview of applicable evidence to persuade you that it is time to focus on OCS stewardship in asthma.
Why discuss OCS stewardship?
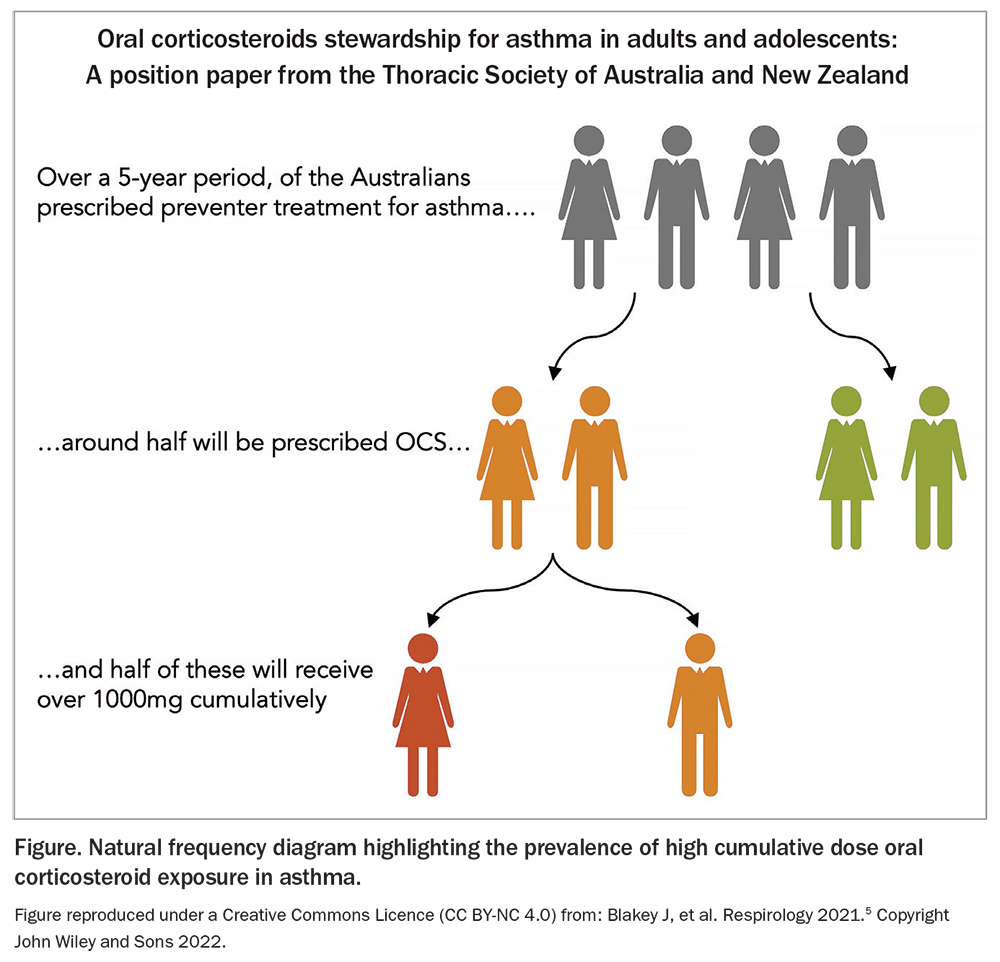
OCS prescription remains extremely common for asthma, particularly in general practice, despite there being little research evidence or objective measurement on an individual level to support this practice. The issue was clearly highlighted in a study conducted in Australia using PBS data, showing that about a quarter of patients prescribed regular inhaled asthma therapy also received at least 1000 mg of prednisolone (or equivalent) over the five-year study period (Figure).3,5 Other recent studies have shown a substantial risk of serious side effects once this dose threshold is exceeded – vital information that has seemingly not been widely recognised.6 These and similar studies suggest that clinicians have prioritised potential short-term gains of OCS over their short- and long-term detrimental impacts.
{kind=link}
The situation pertaining to OCS overuse has some parallels with over-prescribing of antibiotics for viral infections and the potential for developing resistant bacterial strains. This problem with antibiotic overuse has been largely mitigated by the introduction of antimicrobial stewardship initiatives.7 In analogous fashion, we advocate that we now need to consider introducing and propagating OCS stewardship.
What are the benefits of OCS treatment?
A short course of OCS remains a mainstay of treatment for the management of moderate to severe acute exacerbations of asthma in both outpatient and inpatient settings. As OCS are as effective as intravenous or intramuscular corticosteroids, this simplifies their use in the community, avoiding the need for hospital admissions or using health services with specialist nursing care.8 A short course of OCS has been shown to reduce the frequency of persisting severe symptoms during an acute exacerbation whilst reducing the risk of repeat exacerbations.9 In adults, OCS use within the first hour of presenting to the emergency department is associated with a reduced risk of hospitalisation.10 In patients with a history of severe asthma exacerbations and a good understanding of their own asthma management, early initiation of OCS at home may also prevent the development of severe exacerbations and mitigate the need to present to the emergency department.
What are the problems with OCS treatment?
Short-term use of OCS during acute asthma exacerbations is often relatively well tolerated. However, many patients still report side effects, including mood changes, sleep disruptions and gastrointestinal disturbances.11 Additionally, in patients with diabetes, the use of OCS can increase blood glucose levels, which may necessitate more frequent monitoring and an alteration in diabetes management during OCS therapy. Short-term OCS use has also been associated with an increased risk of sepsis, venous thromboembolism and fracture within 30 days of treatment.12
Chronic OCS use, whether in the form of maintenance dosing or high cumulative doses from frequent burst therapy, is associated with significant adverse effects and burden of disease. These long-term complications are well documented and include osteoporosis and fracture, obesity, diabetes, cardiovascular disease, cerebrovascular disease, recurrent infections, adrenal insufficiency and mood disturbances.13 Additionally, patients with higher exposure to OCS have greater healthcare resource use, including more presentations to the emergency department and more frequent inpatient hospital admissions, with resultant higher healthcare costs.14 Although this increased healthcare cost is, in part, driven by asthma disease severity, much of the cost results directly from the adverse effects of OCS.15
Who should receive OCS treatment?
Initial trials of OCS in the mid-to-late 1950s showed impressive results, with 60% of participants gaining a differential benefit over the use of bronchodilators alone.16,17 This understandably led to widespread and rapid adoption of OCS use for asthma treatment. However, any recommendation around OCS use in asthma comes with two significant caveats. First, the trials that showed a reduced risk of hospitalisation or relapse were undertaken in individuals who were sufficiently unwell to attend an emergency department. There is relatively little information on the magnitude of benefit in primary care, where most corticosteroids are prescribed. Indeed, a large study of young children with mild-to-moderate viral wheeze showed no benefit from treatment with oral corticosteroids.18 A persisting concern is that corticosteroids may potentially be prescribed to patients who report breathlessness but lack objective confirmation of airway inflammation or acute obstruction (this may be because they are treated for, but do not have confirmed asthma, or because there is an alternative cause for their symptoms).19 An asthma exacerbation is defined by symptoms and objective measurements. Clinicians should endeavour to always record both to support their use of acute OCS.
The second major issue is that OCS treatment predominantly ameliorates type 2 inflammatory responses. It has been known for more than 50 years that individuals without objective evidence of this do not benefit from chronic OCS treatment. Other therapies now exist that successfully treat this type 2 inflammation without the need for chronic OCS. Maintenance OCS should only be used after multidisciplinary assessment in a specialist asthma clinic. OCS use in other circumstances should be carefully considered by the prescriber, for example OCS treatment may possibly be appropriate when attempting to stabilise a highly symptomatic patient who is awaiting characterisation in a specialist service.
How should OCS treatment be prescribed?
To minimise harm, OCS treatment should be prescribed at no more than the effective dose for no longer than is of proven benefit. Comparisons of different corticosteroid drugs, routes, doses and durations have shown no additional benefit from high-dose or protracted regimens, more potent agents or parenteral administration. Practitioners should continue to prescribe in accordance with the consensus in national and international guidelines: five to seven days of 40 to 50 mg prednisolone.20
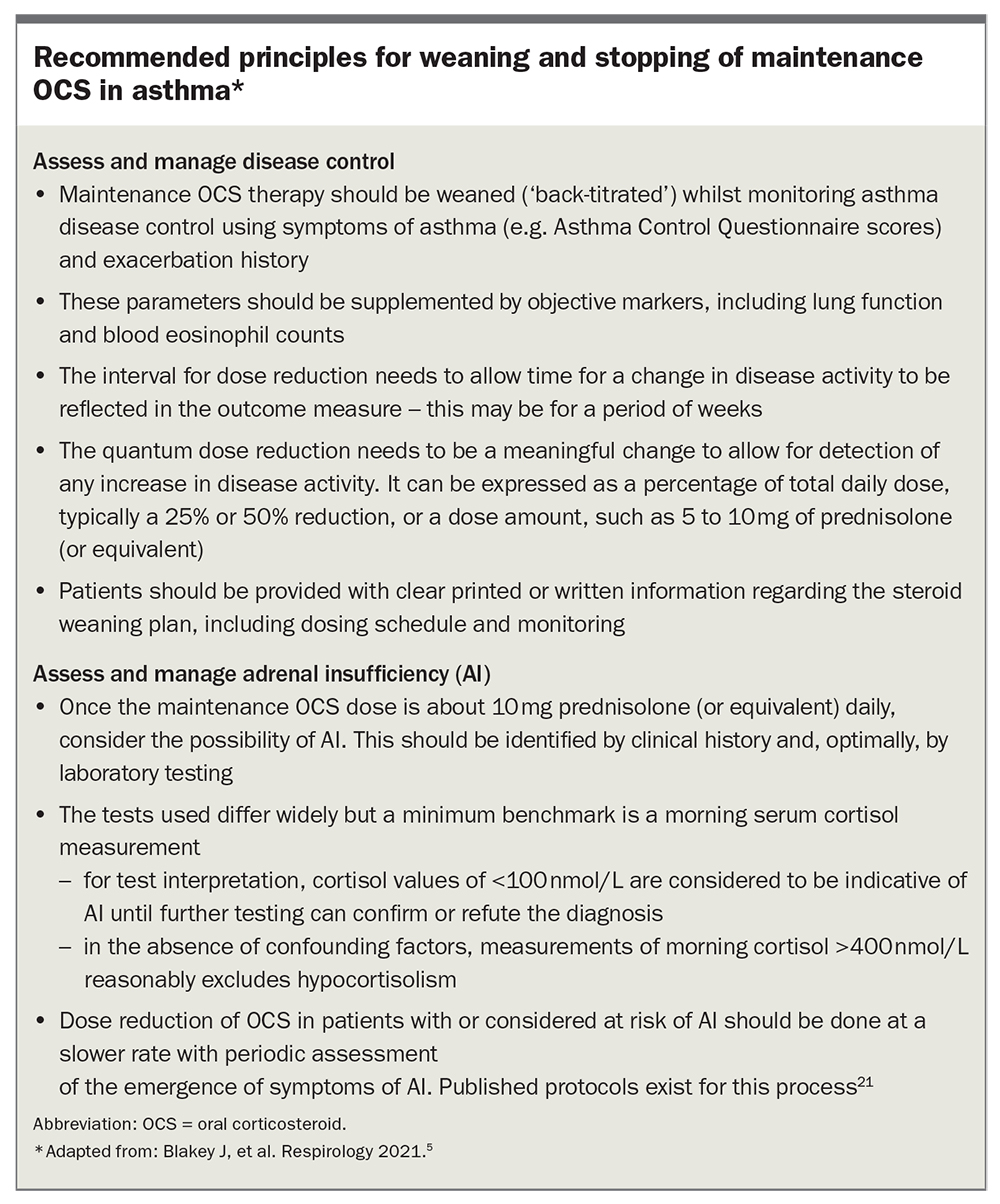
Tapering short-burst corticosteroid courses exposes patients to significantly more corticosteroid (and thus risk of harm) without proven benefit. A further complication in Australia is the common practice of prescribing a standard quantity of prednisolone (30 tablets of 25 mg prednisolone) that exceeds the amount needed for the course (10 to 14 tablets), or pharmacies dispensing this standard amount even if not prescribed. Patients, therefore, often receive two or three times as many tablets as are needed to complete their treatment. This can give the impression that OCS treatment is safe, or that self-administration can be initiated by the patient. It also renders it challenging to determine whether patients have reached the threshold for specialist referral or monitoring, for example the need for bone mineral density scans. Practitioners are encouraged to specify on prescriptions exactly how many tablets are needed for the course rather than the default PBS amount. This should highlight that no more than the prescribed amount should be dispensed. Using the minimum maintenance OCS treatment is essential, and most patients can be successfully weaned off entirely. Principles of OCS weaning are shown in the Box.5,21
{kind=link}
How can we prevent recurrent prescriptions?
An array of interventions have been shown to reduce the risk of future asthma attacks and, thus, the use of OCS treatment. The cornerstone of asthma therapy is the provision of inhaled corticosteroids (ICS). Despite ICS being shown to reduce the risk of death or severe exacerbation by at least half, and consistently being recommended in guidelines, it remains commonplace to see asthma ‘treated’ with bronchodilators alone.22,23 Indeed, the latest iterations of asthma guidelines support the use of as needed (PRN) ICS/formoterol over PRN short-acting bronchodilators.24 The effectiveness of ICS in preventing exacerbations is substantially impaired when patients do not take their inhalers regularly or have poor inhaler technique. Patients with asthma should be prescribed an ICS. A person labelled as having asthma but who only takes salbutamol should have their diagnosis objectively reviewed, and either have ICS added or salbutamol stopped. Regular assessments of adherence and inhaler technique should be undertaken.
Other relatively simple measures can be implemented in primary care to reduce a patient’s risk of requiring OCS treatment. These include smoking cessation support, weight loss management or switching to an ICS/formoterol-containing reliever. The latter strategy for maintenance and reliever therapy is associated with significantly fewer exacerbations and OCS-burst therapy.25
For patients with difficult-to-treat asthma (i.e. uncontrolled symptoms or having exacerbations despite ICS with long-acting bronchodilator therapy), referral for specialist multidimensional asthma assessment leads to a reduction in OCS bursts.26 This may be achieved through the use of highly effective specialist medications, such as monoclonal antibodies, or through the systematic identification of additional pathologies that may be driving symptoms. Unfortunately, most patients who are referred to specialist asthma clinics have experienced many courses of OCS over several years. Most people who are eligible for review are not referred from primary care.27 GPs are recommended to consider referral for specialist care at an earlier stage, for example after two bursts of prednisolone, rather than waiting until significant harm has accrued.
Where can doctors get more information?
The urgent need and rationale for OCS stewardship were recently outlined in a Position Statement supported by the Thoracic Society of Australia and New Zealand (TSANZ).21 This useful resource provides detailed information on key aspects of OCS stewardship. A valuable additional resource that is available to both clinicians and patients is the Severe Asthma Toolkit (https://toolkit.severeasthma.org.au). The toolkit is a unique Australian innovation that permits access to OCS report cards, infographics for chronic OCS use and harms, as well as a patient charter.
Other options to get to know more about OCS stewardship and reducing OCS prescriptions include liaising with respiratory physicians and severe asthma clinics, located in most metropolitan hospitals. The pandemic-inspired development of telehealth platforms makes it possible for rural GPs and asthma nurses to contact respiratory teams and severe asthma clinics directly for advice and to discuss referral of problem cases.
Conclusion
OCS therapy is common and can be highly effective; however, overuse leads to irreversible harm. It is crucial to remember that better control of asthma and less OCS use can almost always be achieved by improved inhaler technique, better adherence to therapy, smoking cessation and optimised medications (including appropriate use of biological therapies). Other initiatives should be pursued and considered for implementation. These may include targeted identification and management of patient comorbidities, restrictions of OCS prescription (e.g. prescribing only 10 tablets of 25 mg prednisolone in a rescue pack rather than 30 tablets) and capturing OCS use for asthma with review of OCS prescription patterns at the general practice, hospital, state and national levels.
Given the prevalence of asthma, the commonplace use of OCS and the existence of effective interventions, OCS stewardship can prevent thousands of avoidable harmful events from occurring each year. RMT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.