Thunderstorm asthma: a rare epidemic

Asthma in children
Thunderstorm asthma is a cause of potentially catastrophic, widespread bronchospasm that can affect many people simultaneously. The causes, management and implications for primary care of this unique phenomenon are reviewed in this article.
- Thunderstorm asthma is a rare event caused by a unique combination of climatic conditions and airborne allergens affecting susceptible people.
- Epidemic asthma can occur, having the potential to affect hundreds of patients across a wide geographical area and placing overwhelming demand on ambulance and health services.
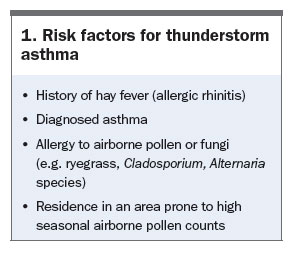
- People considered at risk of thunderstorm asthma are those with seasonal asthma, hay fever or known ryegrass or fungal-spore allergy. Spring predominance has been seen in Australian episodes.
- Strategies to prevent thunderstorm asthma in susceptible people include having an up-to-date asthma action plan, inhaled preventer use and remaining indoors during high-risk days.
- GP management is important to identify and educate at-risk patients, optimise preventive strategies and, potentially, treat acute asthma during outbreaks.
Picture credit: © RapidEye/iStockphoto.com
Model used for illustrative purposes only
Thunderstorm asthma (i.e. thunderstorm-associated asthma) is a rare event whereby aeroallergens in association with thunderstorm activity cause bronchospasm in susceptible people. Incidents occur around the world episodically, about once every few years, and can result in widespread epidemic asthma stressing and potentially overwhelming local health services. Although similar to usual asthma in terms of presentation and treatment, there are unique aetiological factors, preventive recommendations and public health implications to consider. GPs have a role in identifying susceptible patients, counselling and optimising preventive strategies in those at risk and, potentially, managing acute asthma in the primary care setting during outbreaks.
Mechanism of thunderstorm asthma
Thunderstorm asthma is recognised to occur when a unique combination of meteorological and atmospheric conditions coincide. The major aetiological factor is likely to be specific aeroallergens that are greatly amplified in number by storm activity, with grass pollen (specifically ryegrass) most frequently implicated.1 Other airborne particles that have been found to increase in number before thunderstorm asthma epidemics include sporulating fungi such as Cladosporium, Didymella and Alternaria species.2 The resulting increase in airborne allergen load leads to bronchospasm in susceptible individuals.
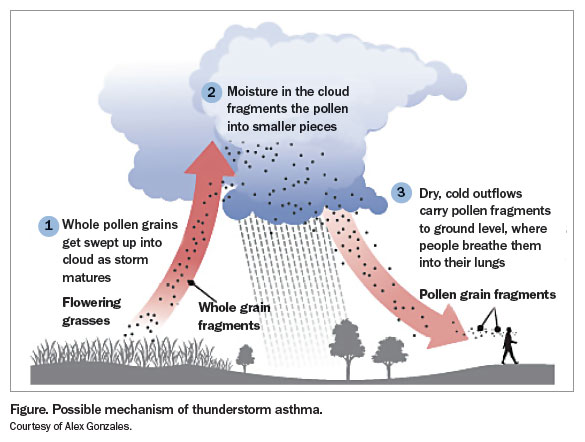
The mechanism of increased aeroallergen load occurring with thunderstorm activity is incompletely understood. Grass pollen grains rupture when exposed to moisture, which has been shown to result in numerous paucimicronic-sized starch particles.2 These particles have aerodynamic properties that enable easy traversing of the upper airways, to subsequently lodge in the lower respiratory tract and trigger rapid development of bronchospasm.1
It is not clear why asthma occurs only in association with certain thunderstorm activity and not routinely with other rain or thunderstorms, even when these coincide with days of high pollen counts. One hypothesis is that outflows of cold air, associated with downdraughts of an approaching thunderstorm, sweep allergenic particles up, concentrating them in a shallow band of air near ground level ahead of the rain front (Figure).3
{kind=link}
Associations with lightning strike densities have also been noted, with a study in England and Wales demonstrating a greater than 50-fold increased risk of epidemic asthma during days of high sferic (lightning) activity.4 Although there is some evidence that changes in the electrical charge on aeroallergen particles can promote their deposition within the alveoli, it is more likely that lightning merely reflects severe thunderstorm activity.5 Increases in humidity have also been associated with episodes of thunderstorm asthma, perhaps as a result of moisture absorption leading to increased rupture of pollen grains, or alternatively, again, as a marker of storm activity.6
Past events
Before 2016, thunderstorm asthma had been reported around the world in countries including the UK, Canada, the USA, Greece and Iran, with affected patient numbers most often ranging from fewer than 10 to many hundreds.2 In Australia, thunderstorm asthma was reported in Victoria in 1984, 1987, 1989 and 2010, always in the month of November, and in Wagga Wagga, NSW, in October 1997.7-9 These Australian events were relatively small in magnitude, affecting between 100 and 300 people. The spring predominance observed likely reflected the high pollen load present in these months, as well as increased thunderstorm activity as a consequence of the warmer surface temperatures required for storm development.
November 2016
On the evening of the 21 November 2016, the largest incident worldwide of thunderstorm asthma occurred in Victoria, Australia. Over 8000 people attended emergency departments around the state, overwhelming the emergency response networks and resulting in activation of disaster plans for many affected health services. This event was also the most deadly incident of thunderstorm asthma on record, with nine possible deaths reported.10 This event eclipsed prior epidemics in magnitude – the largest outbreaks previously had affected 640 people in London in 1994 and 2000 people in Iran in 2013.11,12
Which patients are susceptible?
Although patients with asthma are susceptible during outbreaks of thunderstorm asthma, emerging evidence suggests that many affected patients have little or no history of asthma.2 Instead, patients affected by thunderstorm asthma often have a history of atopy or hay fever. For example, of the 640 patients presenting to London emergency departments in the 1994 outbreak, 44% had no prior asthma diagnosis, yet 63% had hay fever.11 In another English outbreak of thunderstorm asthma affecting 39 patients over an eight-hour period, 33% had no prior diagnosis of asthma, but 57% were regularly affected by hay fever.13 This proportion is similar to the Wagga Wagga episode in 1997, where 36% of 148 cases had not been diagnosed with asthma, yet 90% had experienced hay fever in the preceding 12 months. Even stronger associations with hay fever were observed in the Melbourne events of 1987 and 1989, when 100% of affected patients had hay fever.7
Supporting the association between allergen exposure and thunderstorm asthma, specific allergies have been demonstrated in affected patients, with ryegrass pollen most frequently implicated. In Wagga Wagga, 96% of 148 affected patients were found on skinprick testing to be allergic to ryegrass pollen; affected patients were 23-times more likely to test positive than control patients.9 Cladosporium fungal sensitisation was also found in 61% of cases, three-times more frequently than in controls. A case–control study from a thunderstorm asthma event in Cambridge, England, in 2002 showed patients affected by thunderstorm asthma to be more likely to have sensitisation to Alternaria fungal species and Cladosporium (odds ratios 9 and 3, respectively).14 All Melbourne patients from the 1987 and 1989 events had a positive skin-prick test to ryegrass pollen.7 These findings, combined with data showing increased aeroallergen concentrations during thunderstorm asthma events, suggest aeroallergens are highly likely to have a role in precipitating asthma in susceptible people.11,14
Exposure to outdoor air is associated with risk of bronchospasm in thunderstorm asthma. In the Wagga Wagga outbreak in 1997, people located outdoors had twice the risk of experiencing asthma symptoms during the thunderstorm, compared with people who stayed indoors.9 This provides further evidence for the role of aeroallergens in the precipitation of asthma symptoms (Box 1).
{kind=link}
Inhaled corticosteroids have been found to be protective in case–control studies of thunderstorm asthma events. In Wagga Wagga, after adjustment for variables including age, diagnosed asthma and variables related to asthma severity, affected patients were less than half as likely as controls to be using an inhaled corticosteroid at the time of the thunderstorm asthma outbreak.9 This protective association with inhaled corticosteroid use was also seen in Melbourne patients from the 1987 and 1989 events.7
Management of outbreaks
Epidemic/disaster considerations
Before the November 2016 epidemic, episodes of thunderstorm asthma had demonstrated a significant potential to disrupt health services. In the large London event, 640 patients presented over a 30-hour period to 12 emergency departments (EDs) throughout the greater London area.11 Five patients were admitted to intensive care units; there were no deaths. Five EDs ran out of nebuliser masks, six ran out of beta-agonist inhalers, and eight ran out of oral corticosteroids. Six EDs called in additional doctors and nurses to cope with demand. Despite this, none of the hospitals involved activated their major incident plans.
In the latest Victorian incident, more than 8000 patients presented to emergency departments. The overwhelming demand placed on ambulance services statewide, and deaths that occurred due to the event, were widely reported in the media.
During a thunderstorm asthma event, health services should be prepared for a rapid influx of patients, some of whom will have severe life-threatening bronchospasm. Activation of hospital emergency protocols (e.g. a ‘code brown’) should be considered, to provide extra capacity to accommodate potentially hundreds of patients and to mobilise extra resources. This may include increasing ward capacity to house patients, obtaining extra supplies of metered dose inhalers, spacers and nebulisers from around the hospital, mobilising extra doctors and nurses to help manage patients, and alerting intensive care or retrieval services for assistance with critically unwell patients. Patients are also likely to present to GP clinics, which should be equipped to manage acute bronchospasm and facilitate transfer to hospital of severely affected patients.
Bronchospasm management
Treatment of established bronchospasm in thunderstorm asthma is no different from treatment of other asthma exacerbations. If patients experience wheeze, chest tightness, cough or shortness of breath, they should activate their asthma action plans, and take regular reliever (blue inhaler) medications with a spacer. If symptoms are not abating, early medical attention should be sought.
Management in the clinical setting is similar to any severe asthma exacerbation, and should be based on National Asthma Council guidelines.15 Inhaled salbutamol, supplemental oxygen and pulse oximetry should be instituted, oral corticosteroids administered and depending on response, inhaled ipratropium bromide added. For severe, life-threatening acute asthma, transfer to higher level care, ventilatory support and other therapies may be required. The Asthma Handbook has a printable algorithm titled Managing acute asthma in adults available online (www.asthma handbook.org.au/figure/show/65).
Prevention
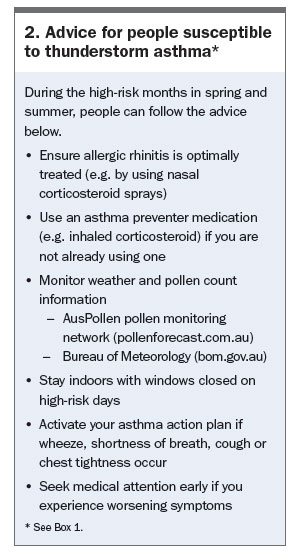
Patients considered susceptible to thunderstorm asthma should be identified and have an asthma action plan in place to minimise the risk of an attack in the event of favourable climatic conditions.16 Patients who experience hay fever should have their allergic rhinitis management optimised, including nasal corticosteroid sprays and/or oral antihistamine medications. For patients with seasonal asthma who develop symptoms predominantly during spring or summer, and particularly those who have a known pollen allergy, regular inhaled corticosteroid use during these susceptible months is recommended. In Melbourne, this is predominantly during October through to the end of December. Patients should be encouraged to follow pollen counts and weather advice and on high-risk days they should remain indoors with windows closed. For selected patients with severe allergic rhinitis or pollen-induced bronchospasm, desensitisation (allergen immunotherapy) can be explored – in these cases, referral to an immunologist or respiratory physician is recommended. Advice for people susceptible to thunderstorm asthma is summarised in Box 2.
{kind=link}
Given the severity of the Victorian thunderstorm asthma epidemic in November 2016 and the worldwide distribution of thunderstorm asthma, there is much interest in developing predictive models for future events. Adequate prediction tools would enable susceptible patients to activate asthma action plans and allow health services to start disaster planning to mitigate the risk of overwhelming demand on ambulance and hospital services. Currently, such predictive ability is hampered by difficulty in identifying which thunderstorms are associated with cold air outflows sufficient to concentrate a layer of air ahead of the approaching rain front.3 Due to the frequency of thunderstorms over spring and summer, disaster planning for every forecast storm event is impractical. Future research should concentrate on exploring the correlation between specific climatic conditions, aeroallergen load and patient symptoms to help refine predictive models.
Conclusion
Thunderstorm asthma is an infrequent but potentially catastrophic phenomenon. GPs have an important role to play in identifying patients at risk, which includes those with hay fever and/or seasonal asthma. Management of these patients in the primary care setting includes ensuring an up-to-date asthma action plan is in place, using inhaled corticosteroids for prevention and providing advice on how to avoid developing asthma during high-risk days. Referral to an immunologist or respiratory specialist should be considered in severe cases of allergic rhinitis. GPs should also ensure they have adequate resources to manage acute bronchospasm in the clinic setting. RMT
References
- Suphioglu C, Singh MB, Taylor P, et al. Mechanism of grass-pollen-induced asthma. Lancet 1992; 339: 569-572.
- Dabrera G, Murray V, Emberlin J, et al. Thunderstorm asthma: an overview of the evidence base and implications for public health advice. QJM 2013; 106: 207-217.
- Marks GB, Colquhoun JR, Girgis ST, et al. Thunderstorm outflows preceding epidemics of asthma during spring and summer. Thorax 2001; 56: 468-471.
- Newson R, Strachan D, Archibald E, et al. Acute asthma epidemics, weather and pollen in England, 1987-1994. Eur Respir J 1998; 11: 694-701.
- O’Leary M, Koolpiruck D, Balachandran W, Emberlin J, Lewis R. The role of electrostatic charge accumulated by respirable sized allergens with regard to thunderstorm asthma. Fourtieth Industry Applications Society Annual Meeting, Industry Applications Conference: Conference Record of the 2005 Industry Applications Conference; 2005. Pp. 778-783.
- Celenza A, Fothergill J, Kupek E, Shaw RJ. Thunderstorm associated asthma: a detailed analysis of environmental factors. BMJ 1996; 312: 604-607.
- Bellomo R, Gigliotti P, Treloar A, et al. Two consecutive thunderstorm associated epidemics of asthma in the city of Melbourne. The possible role of rye grass pollen. Med J Aust 1992; 156: 834-837.
- Howden ML, McDonald CF, Sutherland MF. Thunderstorm asthma – a timely reminder. Med J Aust 2011; 195: 512-513.
- Girgis ST, Marks GB, Downs SH, et al. Thunderstorm-associated asthma in an inland town in south-eastern Australia. Who is at risk? Eur Respir J 2000; 16: 3-8.
- Review of response to the thunderstorm asthma event of 21–22 November 2016 Preliminary Report. Inspector-General for Emergency Management, 121 Exhibition Street, Melbourne. 2016. Available online at: http://www.igem.vic.gov.au/home/reports+and+publications/reports (accessed April 2017).
- Davidson AC, Emberlin J, Cook AD, Venables KM. A major outbreak of asthma associated with a thunderstorm: experience of accident and emergency departments and patients’ characteristics. Thames Regions Accident and Emergency Trainees Association. BMJ 1996; 312: 601-604.
- Forouzan A, Masoumi K, Haddadzadeh Shoushtari M, et al. An overview of thunderstorm-associated asthma outbreak in southwest of Iran. J Environ Public Health 2014: 504017.
- Campbell-Hewson G, Cope A, Egleston CV, et al. Epidemic of asthma possibly associated with electrical storms. BMJ 1994; 309: 1086-1087.
- Pulimood TB, Corden JM, Bryden C, et al. Epidemic asthma and the role of the fungal mold Alternaria alternata. J Allergy Clin Immunol 2007; 120: 610-617.
- National Asthma Council Australia. Australian Asthma Handbook Version 1.2, Melbourne; National Asthma Council Australia, 2016. Available online at: http://www.asthmahandbook.org.au (accessed April 2017).
- The Australasian Society of Clinical Immunology and Allergy (ASCIA). Thunderstorm asthma: information for patients, consumers and carers. Available online at: https://www.allergy.org.au/patients/asthma-and-allergy/thunderstorm-asthma (accessed April 2017).