Severe refractory asthma. The promise of new treatments

Professor Katelaris is Head of Unit, Immunology and Allergy at Campbelltown Hospital; and Professor of Immunology and Allergy at Western Sydney University, Sydney, NSW.
Asthma
Asthma in children
Several biological therapies have recently been developed targeting specific pathways of inflammation in asthma. Although they have the potential for greater therapeutic benefit than standard therapies in poorly controlled patients, they require reliable identification of the appropriate patient for each particular biological therapeutic approach.
- In Australia, asthma affects about 10% of people, and about 5% of these have severe asthma.
- Severe asthma is associated with significant morbidity and is a considerable burden to both the individual and the community.
- New treatment strategies are required to lessen the burden of this disease, which includes frequent exacerbations, hospitalisation, corticosteroid use and poor quality of life.
- Asthma is regarded as a heterogeneous disorder with distinct phenotypes.
- Over the past two decades significant advances have been made in our understanding of the molecular mechanisms underpinning the various types of asthma. This has led to the development of several biological therapies that are more precisely targeted to antagonise key molecules in the inflammatory process.
Severe asthma affects about 5% of the asthma population, is associated with significant morbidity and is a considerable burden to both the individual and the community. Severe asthma is a term used to describe asthma that is inadequately controlled despite the use of maximal doses of inhaled corticosteroids (ICS) and long-acting beta agonists (LABA), or requires oral corticosteroids in addition to inhaled therapy to gain control. In people who have these characteristics, it is important to review the diagnosis and consider alternative diagnoses. Most patients with asthma do not have severe disease once they are carefully evaluated and their treatment is optimised. If this has been done, then attention to comorbidities such as smoking, obesity, aspirin sensitivity and nasal polyposis may also positively impact disease control.
The key features of severe asthma are poor symptom control and suboptimal lung function. Patients with severe asthma also experience:
- significant disease burden that includes exposure to and side effects from high-dose ICS and oral corticosteroid use
- hospitalisations and emergency department visits for exacerbations
- work or school loss.
Suboptimal lung function is a risk factor for oral corticosteroid use and more hospitalisations. Management of severe asthma in primary care has recently been reviewed in Medicine Today.1 This article focuses on the new therapeutic modalities available after specialist referral and assessment.
Immune mechanisms in asthma
Asthma is a chronic inflammatory disease of the airways manifesting as bronchial hyper-reactivity and episodic symptoms of airflow obstruction. In the long term there may be airway remodelling leading to fixed airways obstruction. Various characteristics such as certain symptom complexes, environmental triggers or, more recently, specific biomarkers can be used to define various asthma categories or phenotypes. Classifying asthma based on cellular inflammation phenotypes highlights the heterogeneity of the disease.
Over the past two decades significant advances have been made in our understanding of the molecular mechanisms underpinning the various types of asthma. This has led to the development of several biological therapies that are more precisely targeted to antagonise key molecules in the inflammatory process. Various subtypes of asthma may be expected to respond differently to these targeted therapies, so the challenge has become one of identification of the appropriate patient for a particular biological therapeutic approach.
The presence of eosinophils is indicative of what is termed the type 2 (T2) inflammation phenotype whereby the key cytokines responsible for inflammation are interleukin(IL)-4, IL-5 and IL-13 (T helper 2 [Th2]-specific cytokines). At this stage, immune mechanisms and molecular targets are better defined for the T2 phenotype than for other phenotypes although nonT2 subtypes may result in severe asthma as well.2 Identification of the T2 phenotype by the use of certain biomarkers has been an intense area of research.
Biomarkers
An ideal biomarker must be easy to collect in a noninvasive fashion, measure and store. In addition testing must be economical and reliable with high sensitivity. A biomarker may be used to guide choice of a particular treatment or to monitor treatment effect, appropriate dosing and adherence. A number of markers have been investigated as features of T2 airways inflammation, including immunoglobulin E (IgE) levels, fractional exhaled nitric oxide (FeNO) levels, serum periostin levels, and sputum and blood eosinophil counts. The first example of using biomarkers to predict therapy in severe asthma comes from the development of mepolizumab, a humanised monoclonal antibody against IL-5.
New and emerging therapies
There are several new immune response modifiers targeting specific pathways of inflammation. Although they have the potential for greater therapeutic benefit than standard therapies in patients with poorly controlled asthma, they require reliable identification of the particular target population. There are now several monoclonal antibodies targeting key molecules in T2 inflammation, including IgE, IL-4, IL-5, IL-13 and thymic stromal lymphopoietin (TSLP) (Figure 1).3
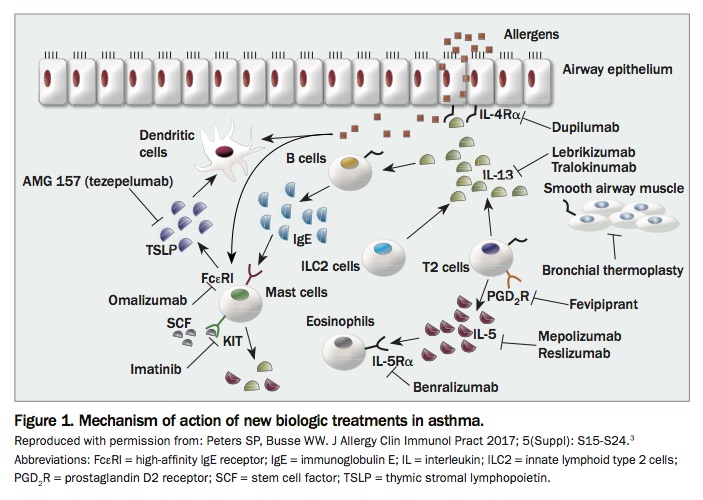{kind=link}
Anti-IgE therapy: omalizumab
Omalizumab is a humanised monoclonal antibody against IgE, binding circulating IgE, regardless of specificity, via the C3 region of the molecule. By blocking binding of IgE to the high-affinity receptor on mast cells and basophils, omalizumab causes down regulation of the receptor and limits the degree of mediator release.
Multiple phase III studies and a number of postmarketing observational real-life studies have shown a beneficial impact of omalizumab on asthma exacerbations, consistent reductions in rates of unscheduled outpatient visits, reduced hospitalisations for asthma, significant reductions in asthma symptoms and improvements in quality of life. Significant reduction in use of ICS has also been shown.4-8
Omalizumab has a good safety profile with an adverse event rate comparable with other treatments. In the omalizumab clinical trial programme leading to its registration, three of 3507 (0.1%) patients experienced anaphylaxis. This occurred with the first dose in two patients and with the fourth dose in one patient. The time to onset of anaphylaxis was 90 minutes after administration in two patients and two hours after administration in one patient.9 An observation period of two hours is now recommended for the first two doses of omalizumab, which must be given in a facility that has adequate resuscitation facilities for the management of anaphylaxis.
Omalizumab was registered in Australia in 2002 and is indicated for the management of severe allergic asthma in children and adults in whom there is inadequate control despite high-dose ICS use. It is also subsidised on the PBS for eligible individuals who must have evidence of reversibility on respiratory function tests and specific IgE reactivity to aeroallergens demonstrated by skin tests or in vitro measures. It is dosed according to body weight and total IgE level. Tables for dose calculation are available in the product information.
Anti-IL-5 and anti-IL-5R therapies: mepolizumab, reslizumab and benralizumab
Eosinophilic inflammation in asthma is associated with more frequent exacerbations and declining lung function. IL-5 is a type 2 cytokine, produced by Th2 cells and type 2 innate lymphoid cells and operates via the alpha subunit of the IL-5 receptor (IL-5Rα) found on eosinophils and some basophils. IL-5 is a key cytokine in eosinophil maturation, activation and survival (Figure 2).10,11
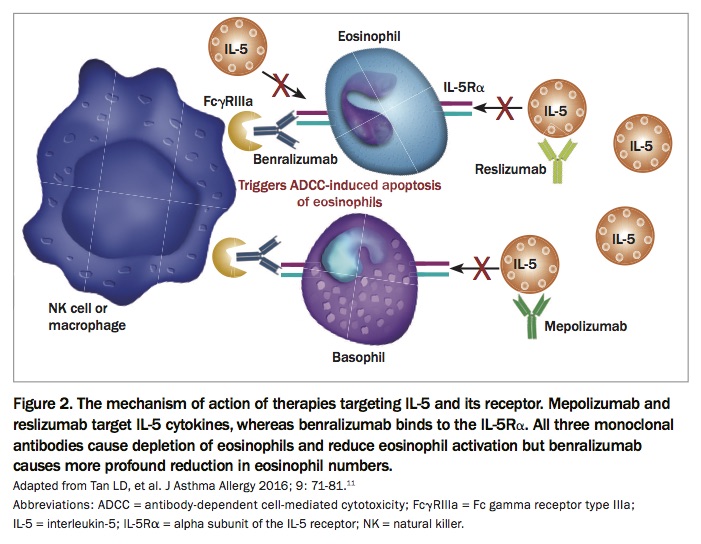{kind=link}
Mepolizumab is a monoclonal antibody directed against IL-5.11 It has been shown to reduce asthma exacerbations by about 50%, improve lung function and reduce the need for oral corticosteroids without loss of control.12,13 Mepolizumab is subsidised on the PBS for eligible patients with severe eosinophilic asthma and a blood eosinophil count of 300 cells per microlitre or higher. It is given by monthly subcutaneous injection at a fixed dose of 100mg.
Reslizumab is another monoclonal antibody directed against IL-5. It has shown efficacy in phase III trials in patients with asthma and high peripheral eosinophil counts. It reduces exacerbation frequency and improves quality of life, asthma control and lung function.14 It is approved by the TGA in Australia as add-on therapy in patients with eosinophilic asthma. It is given as an intravenous injection.
Benralizumab is a humanised monoclonal antibody directed against the alpha subunit of the IL-5 receptor (IL-5Rα). It induces rapid and near complete depletion of eosinophils by natural killer cell-mediated antibody-dependent cellular cytotoxic effects, thereby acting as a potential asthma therapeutic. There have been five studies comparing benralizumab with placebo involving over 3000 patients. Benralizumab has been shown to reduce asthma exacerbations in adults with uncontrolled eosinophilic asthma and a baseline blood eosinophil count of 300 cells per microlitre or higher.15 Benralizumab has also been shown to reduce the oral corticosteroid dose in patients with severe asthma.16 In Australia, benralizumab has recently been approved by the TGA as add-on therapy in patients aged 12 years and older with severe eosinophilic asthma. It is also registered in the USA and Europe. It is given as a fixed dose subcutaneously monthly at first and may then be administered every eight weeks.
A recent Cochrane review of therapies that target IL-5 or the IL-5 receptor concluded that all three therapies have been examined in high-quality studies and are efficacious as adjunct treatment to standard asthma therapies in patients with severe eosinophilic asthma. These treatments reduced asthma exacerbations by about 50%, with no excess serious adverse events.17
Anti-IL-13 therapies: lebrikizumab and tralokinumab
IL-13 induces eosinophil recruitment to the lung tissue and was shown to be a crucial component of eosinophilic inflammation over a decade ago, making it an attractive target for novel therapies.
Lebrikizumab, an IgG4 humanised monoclonal antibody, has been investigated in a randomised, placebo-controlled, double-blind trial in 219 adults with asthma uncontrolled on ICS.18 The primary outcome, improvement in forced expiratory volume in one second (FEV1) from baseline to 12 weeks, was met and patients with a high baseline periostin level showed the most significant improvement.
Another anti-IL-13 monoclonal antibody, tralokinumab, did not improve symptoms but resulted in a nonsignificant increase in FEV1 compared with placebo.19 Neither of these drugs have gone forward in clinical trials and they are not approved for use in Australia.
Anti-IL-4 and anti-IL-13 therapy: dupilumab
IL-4 and IL-13 play key roles in the pathophysiology of asthma from driving chronic airways inflammation and induction of bronchial hyper-reactivity to tissue remodelling, making them attractive targets for therapeutic interventions.
Although studies targeting IL-13 have shown this to be a target for asthma treatment, there have been limitations to this strategy, no doubt due to the overlapping functions of IL-4 and IL-13. Thus a monoclonal antibody that can block the effects of both cytokines can be expected to have a greater therapeutic effect. Dupilumab is a fully human monoclonal antibody directed against the alpha subunit of the IL-4 receptor; it is therefore capable of blocking the signal pathways activated by both IL-4 and IL-13.20
In a phase II study of patients with moderate-to-severe asthma and peripheral or sputum eosinophilia, there was an 87% reduction in asthma exacerbations with use of dupilumab compared with the placebo-treated group. Significant improvements were also observed in the asthma control questionnaire score and FEV1.21 In a phase IIb trial that enrolled patients with poorly controlled asthma despite high-dose ICS and LABA therapy, dupilumab given as 300mg every two weeks decreased asthma exacerbation rates, the extent of which was dependent on the peripheral eosinophil count. For patients with an eosinophil count of at least 300 cells per microlitre, reduction in exacerbations was between 71 and 81%, and for eosinophil counts less than 300 cells per microlitre, 60 and 68%. Dupilumab, given every two weeks, also improved prebronchodilator FEV1 compared with placebo in all patients, with the greatest effects in those with blood eosinophil counts of 300 cells per microlitre or more.22 Phase III studies are underway with this promising molecule.
Dupilumab has been shown to be effective in the treatment of nasal polyposis and atopic dermatitis and has been registered recently in Australia for this latter indication.
Anti-TSLP: tezepelumab
TSLP is a cytokine that acts upstream in T2 responses, having effects on lymphocyte maturation by its activation of antigen-presenting cells.
Tezepelumab is an IgG2 anti-TSLP human monoclonal antibody undergoing clinical trials. In a phase 2, proof-of-concept, dose-ranging randomised, double-blind, placebo-controlled trial, three doses of the drug, administered subcutaneously, were compared with placebo over a 52-week treatment period in patients with uncontrolled asthma despite medium- to high-dose ICS and LABA. As in other studies, the primary end point was annualised exacerbation rate at week 52. Exacerbation rates were lower by 61% (70mg four weekly), 71% (210mg four weekly) and 66% (280mg two weekly) than the rate in the placebo group (p<0.001 for all groups). Prebronchodilator FEV1 at week 52 was higher than commencement values in the three actively treated groups. Importantly, improvement occurred independent of eosinophil count at enrolment.23 Several biomarkers, including IgE, blood eosinophil count and FeNO, were reduced by week four in the tezepelumab-treated groups. Five patients receiving active drug and one receiving placebo discontinued because of adverse events. One patient on low-dose drug developed pneumonia and a stroke and died and one patient in the medium-dose group developed Guillain–Barre syndrome. Injection site reactions occurred in about 3% of the study population. There were no reports of anaphylaxis. Further trials are underway.23
CRTh2 antagonist: fevipiprant
Fevipiprant inhibits another driver for T2 type inflammation in asthma, the prostaglandin DP2 receptor – also known as the chemoattractant receptor-homologous molecule expressed on Th2 cells (CRTh2). It is under investigation as early studies have shown efficacy. Unlike the currently available monoclonal antibodies, it is an oral preparation taken twice daily.24
Treatment of other asthma endotypes
There is no targeted therapy for noneosinophilic asthma available as yet. Low-dose macrolide antibiotics that can reduce airway neutrophils have been examined in an Australian study using low-dose azithromycin. Fewer exacerbations and improved quality of life were demonstrated in the actively treated group and, surprisingly, this was independent of eosinophil blood counts.25 Further research is needed to better define the noneosinophilic asthma endotypes.
Conclusion
Traditionally, asthma has been defined by clinical and physiological variables, which encompass multiple phenotypes that historically have been treated with nonspecific anti-inflammatory therapies such as corticosteroids.
Recent molecular and genetic studies have identified phenotypes that associate with specific biomarkers, the best studied of which are markers of T2 inflammation including total serum IgE levels, sputum and blood eosinophil count, FeNO levels and periostin levels. The new therapies, although undeniably effective, are currently very expensive, so it is important to have directed patient selection based on T2 signature to ensure cost-effective use.
Cytokine and signalling pathways in noneosinophilic, low T2 subtypes of asthma are less well defined and require further study to allow the development of targeted therapies for this group.
There remain unanswered questions to be addressed to fully understand the place of these new therapies in our treatment algorithms. Most offer a management strategy but are not disease-modifying and there are no head-to-head comparisons between the various treatments, particularly the anti-IL-5 therapies. Apart from omalizumab, which has been in clinical use for 16 years, the remainder are very new, and long-term, real-life data collection will be important to consolidate confidence regarding safety profiles. RMT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.