Obstructive sleep apnoea: assessment and management in general practice

Breathing problems
Obstructive sleep apnoea (OSA) is a prevalent disorder managed in Australian general practice. This article aims to provide an overview of the presenting symptoms, assessment, management and referral options for patients with OSA.
- Obstructive sleep apnoea (OSA) is a prevalent, debilitating and costly disorder that is underdiagnosed and undertreated.
- Presenting symptoms vary considerably between individuals, and the most common risk factors are age, overweight or obesity and male sex; however, OSA also occurs in women, especially after menopause.
- GPs may help patients manage snoring and provide lifestyle advice regarding healthy sleep, diet and physical activity.
- GPs can use brief questionnaires to identify patients with a high risk of OSA and refer them for an overnight sleep study (home-based or laboratory), or to a specialist sleep physician (for patients with severe OSA or significant comorbidities).
- The most reliably effective treatment for moderate and severe OSA is continuous positive airway pressure (CPAP) therapy combined with lifestyle and weight-management advice.
- Patients treated with CPAP should be provided immediate and ongoing support to adapt to CPAP therapy and overcome any barriers to adherence.
- Other treatments, including positional therapy, dental devices and surgery, can be effective and can be used in combination with CPAP; they may be considered depending on the nature and severity of OSA or if the patient does not tolerate CPAP.
Obstructive sleep apnoea (OSA) is a prevalent disorder that is associated with frequent narrowing (hypopnoea) and collapse (apnoea) of the upper airway during sleep. These respiratory events result in reduced oxygen saturation, increased cortical arousals and sleep fragmentation.1,2 OSA is associated with daytime impairments (e.g. sleepiness, fatigue), cardiovascular disease, diabetes, reduced quality of life and increased risk of depression.3,4,5 It affects about one billion people worldwide.6 It is estimated that 20% of the Australian adult general population have at least moderate OSA and 4% have symptomatic OSA (i.e. OSA syndrome with associated symptoms such as daytime sleepiness and cardiometabolic comorbidities).7-10 OSA is underdiagnosed, and untreated OSA is estimated to cost Australia $21 billion annually in direct and indirect economic costs.11
Overview of OSA in primary care
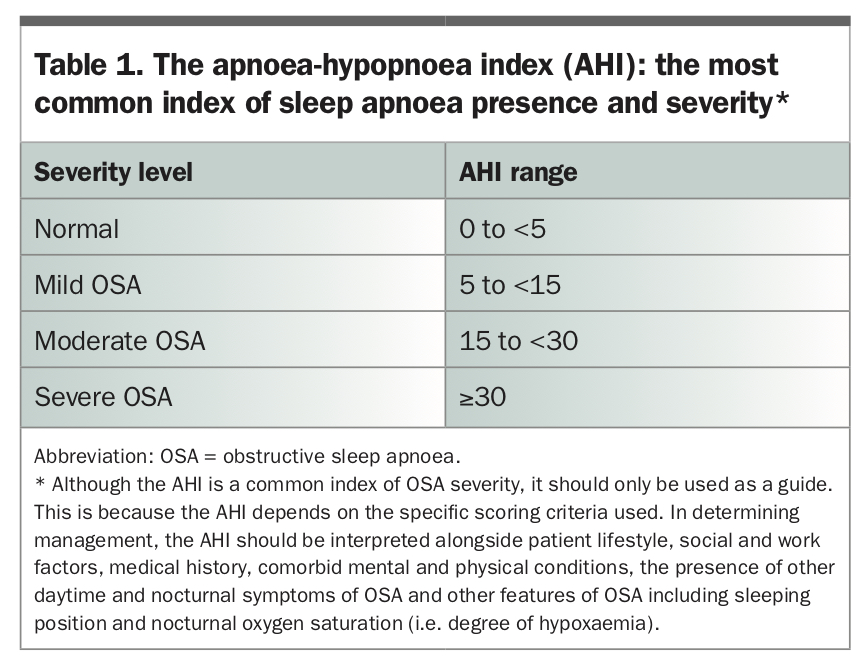
GPs can use simple screening tools to identify patients with a high risk of OSA and refer them for overnight polysomnography (a ‘sleep study’). Overnight polysomnography is the gold standard tool for assessing OSA. The most common index of OSA presence and severity is the apnoea-hypopnoea index (AHI), which reflects the average number of apnoeas and hypopnoeas experienced per hour of sleep (Table 1).
{kind=link}
There are several evidence-based management approaches for OSA that should be guided by severity; features of the condition (e.g. supine-predominant OSA, daytime symptoms); patient history, lifestyle and treatment preference; the presence of motor-vehicle or workplace accident risk; comorbid sleep, physical and mental health conditions; and the availability of treatment options (e.g. in rural and remote settings).12 The most effective treatment for moderate and severe OSA is continuous positive airway pressure (CPAP) therapy (a device worn by the patient during sleep that delivers pressurised air via a face mask to splint open the upper airway) combined with lifestyle and weight-management advice.2,13 However, many patients reject CPAP therapy or discontinue it over time.14 GPs may support patients in overcoming barriers to CPAP adherence. Patients who do not tolerate CPAP therapy may be referred for consideration of second-line management approaches, such as mandibular advancement splints (MAS). It is important for GPs to identify patients with complex presentations of OSA and/or comorbid conditions who may require referral to a specialist sleep physician.
Risk factors for OSA
OSA results from a combination of anatomical and nonanatomical factors. Anatomical factors include airway size, surrounding soft-tissue structures and craniofacial structure. Nonanatomical factors include an increased likelihood of awakening to a small respiratory disturbance, the body’s response to changes in oxygen and carbon dioxide levels during respiratory events and patterns of upper airway muscle tone.15 The most common risk factors for OSA include male sex, overweight or obesity and older age. Although the prevalence of OSA is higher among men, OSA also occurs in women, especially after menopause, but women are less likely to be diagnosed and treated than men.16 The prevalence of OSA increases with age, particularly from 50 years.17 Other risk factors for OSA include excessive alcohol consumption, smoking, sleeping in a supine position, tonsillar hypertrophy, nasal obstruction, craniofacial abnormalities, neuromuscular disease and genetic factors (family history) related to jaw morphology.12 Obesity is a key modifiable risk factor for OSA. GPs may provide patients with lifestyle, weight management and healthy sleep advice as an effective adjunct to other treatment options.12
Comorbid conditions and associated factors
OSA frequently co-occurs with other sleep, mental health and physical conditions. Common comorbidities of untreated OSA include hypertension, coronary artery disease, heart failure, atrial fibrillation, cerebrovascular accidents, type 2 diabetes, mood disorders including depression, cognitive dysfunction and insomnia.4,18-20 Untreated OSA may increase the risk of hypertension, cardiovascular disorders, diabetes and depression.3-5,21
Around 30 to 50% of patients with OSA report clinically significant symptoms of comorbid insomnia (self-reported difficulties initiating and/or returning to sleep).22 Patients with comorbid insomnia and sleep apnoea experience greater morbidity and are more difficult to treat compared with patients with OSA alone.18,23,24
Presentation
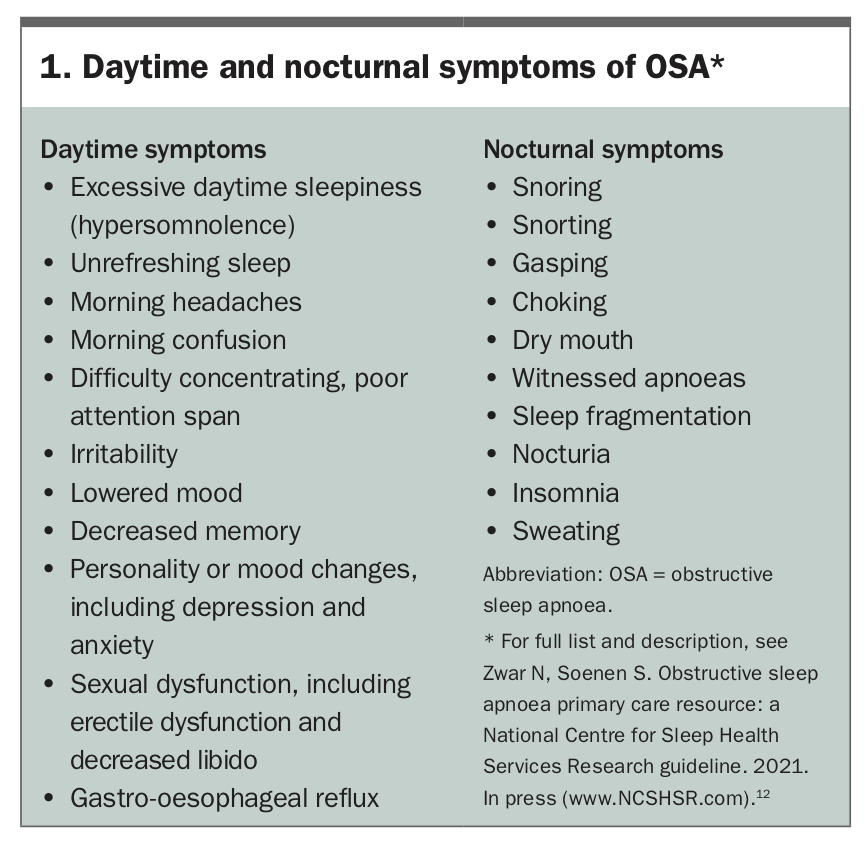
Patients with OSA may present with nocturnal sleep-related and/or daytime symptoms (Box 1).12 Many people with OSA do not report obvious nocturnal symptoms of OSA such as witnessed apnoea events, or daytime symptoms such as excessive daytime sleepiness. This can result in high rates of undiagnosed OSA in the community.25 Consequently, a degree of clinical suspicion is recommended when screening patients for possible OSA.
{kind=link}
Assessment and diagnosis of OSA
OSA is often undiagnosed.7 This results in significant morbidity as well as economic and safety costs.11 It is important for GPs and other primary healthcare workers to understand the risk factors, heterogeneous range of presenting symptoms and management pathways for OSA.
Fitness to drive
People with untreated OSA are at increased risk of being involved in motor-vehicle accidents.26 It is important to assess a patient’s level of risk of having an accident related to sleepiness, including factors such as:
- high-risk occupation (commercial driver or working with heavy machinery)
- severe daytime sleepiness (Epworth Sleepiness Scale score of ≥16/2427)
- self-reported sleepiness while driving
- a history of sleepiness-related motor-vehicle accidents.
Patients at high risk of motor-vehicle and occupational accidents due to sleep apnoea should be referred to a specialist sleep physician and advised to avoid driving if they feel sleepy until receiving further help to manage their condition.
Patient self-report
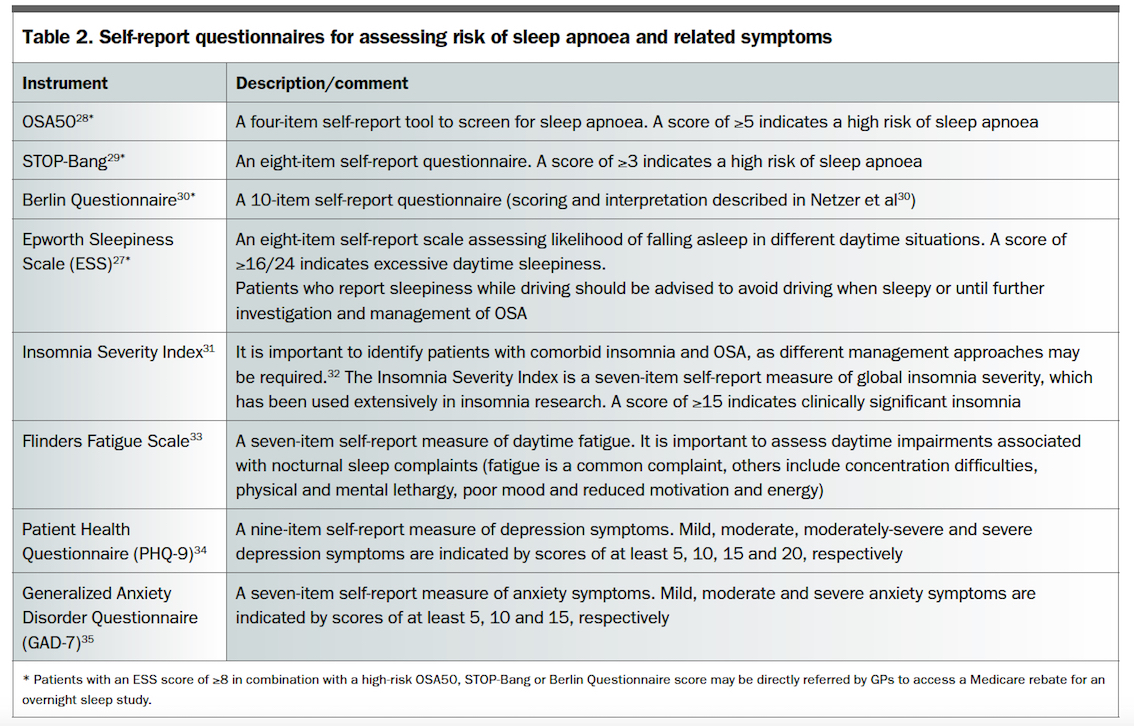
Simple self-report tools can be used in general practice to screen for people at high risk of OSA and related symptoms (Table 2).28-35 These should be used in addition to patient self-reported sleep history (insomnia symptoms, previous sleeping difficulties, comorbid mental/physical conditions and family history of OSA), sleep patterns (total sleep time, time in bed, sleep hygiene behaviours), daytime symptoms (sleepiness, fatigue, depression), diet, exercise and other physical and mental health conditions.
{kind=link}
Screening and referral for sleep studies
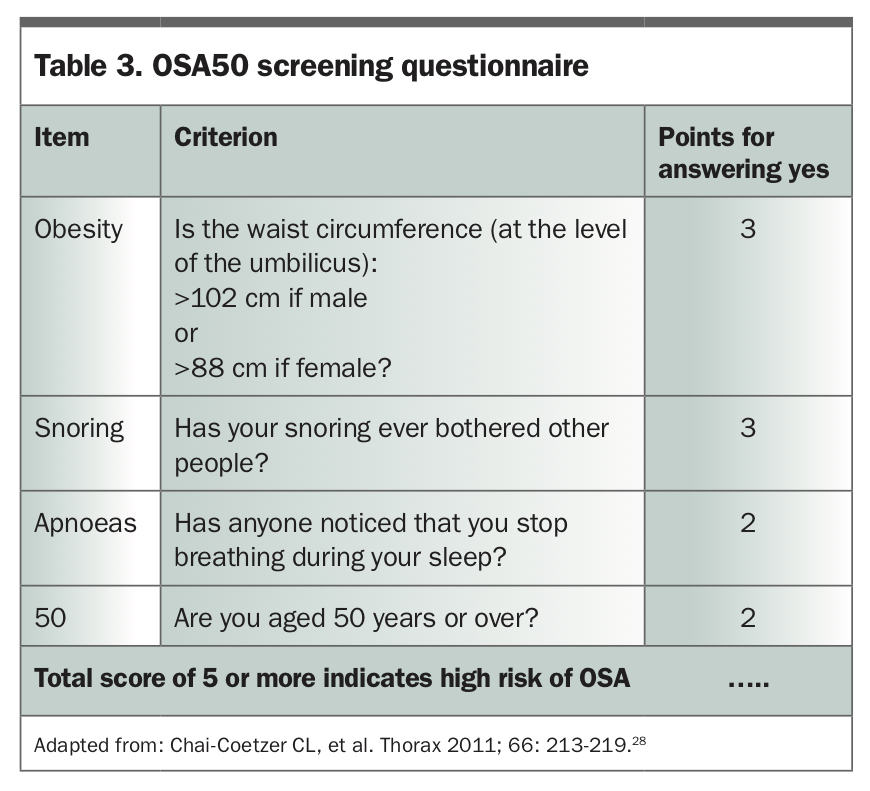
The four-item OSA50 questionnaire (Table 3) and the eight-item STOP-Bang questionnaire (www.stopbang.ca/osa/screening.php) may be used in primary care to identify patients at high risk of OSA.28,29 Australian general population studies indicate that OSA50 and STOP-Bang have adequate sensitivity in identifying patients with clinically relevant OSA (86% and 81%, respectively) but have poor specificity to correctly rule out OSA (21% and 36%, respectively).36 The Epworth Sleepiness Scale is an eight-item self-report measure of likelihood of falling asleep in different daytime situations.27
{kind=link}
Recent Medicare Benefits Schedule item numbers allow GPs to identify patients with a high risk of OSA and refer them directly for an overnight sleep study with a Medicare rebate (OSA50 ≥5, or STOP-Bang ≥3, or ‘high risk’ Berlin Questionnaire result, and an Epworth Sleepiness Scale score ≥8). Patients who do not meet criteria for a GP referral for a sleep study may still have moderate or severe OSA, that is not associated with increased daytime sleepiness, but requires further investigation.
Overnight polysomnography is the gold-standard measure of OSA presence and severity. Patients can undergo polysomnography studies in sleep laboratories or at home. Level 1 studies are conducted in public and private hospitals or sleep clinics and are attended by a trained sleep technologist. Level 2 studies are unattended and use portable recording equipment set up in a sleep clinic or in a patient’s home on the evening of the study.
Polysomnography recording includes a continuous electroencephalogram (brain wave), electromyogram (muscle activity), electrocardiogram (heart rate), electro-oculogram (eye movements), oronasal thermistor (to assess oronasal airflow) and measures of nasal pressure (to assess nasal flow), oxygen saturation, leg movement, body position (supine, prone, lateral) and respiratory effort. Sleep study data are scored by trained sleep technicians according to predefined criteria.37
Level 1 sleep studies may be suitable for patients with suspected OSA and multiple comorbid physical or mental health conditions, children and adolescents, rural and remote patients who do not have access to accommodation near sleep laboratories and patients who require (next day) daytime testing for licensing issues such as sleepiness-related motor-vehicle accident risk. Level 2 sleep studies may be suitable for patients who do not require nursing assistance, those without significant comorbidities and those who can easily attend a sleep laboratory on the evening of the set-up appointment or return portable equipment the next day.
Portable, limited-channel level 3 and 4 sleep study devices (e.g. with airflow and oxygen saturation measures) may be useful in patients with suspected mild-to-moderate OSA according to questionnaire scores, but no evidence of severe OSA, excessive daytime sleepiness, significant comorbid conditions, or in people who drive for work. Level 3 and 4 sleep studies may also be useful as an initial sleep assessment in rural and remote settings in which access to polysomnography services is limited. No MBS reimbursement is currently available for level 3 and 4 sleep studies.
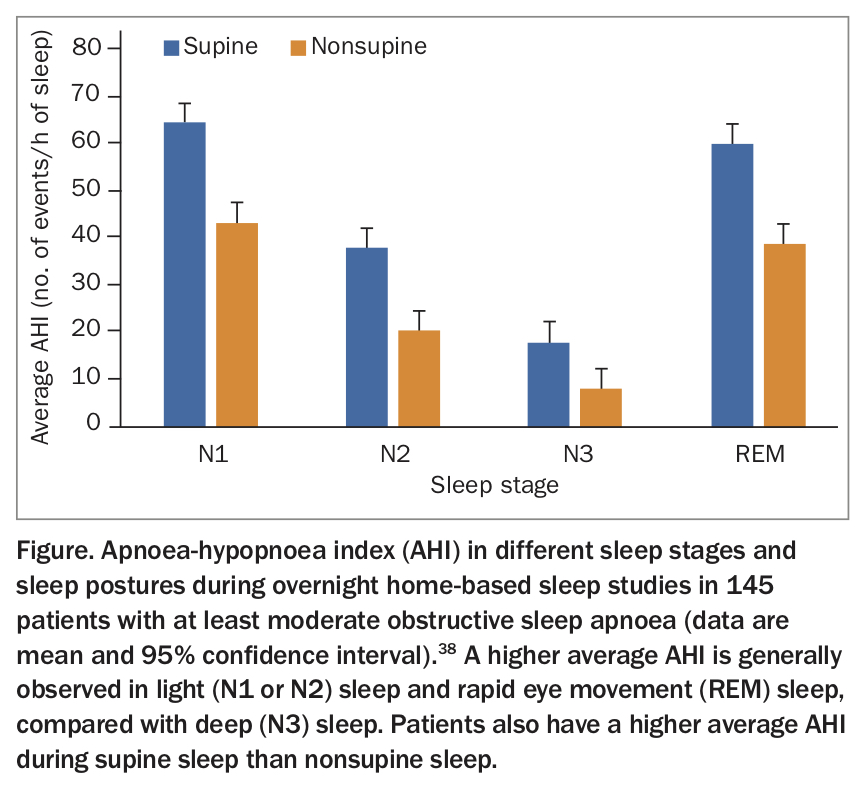
The AHI is the main index of OSA presence and severity (Table 1) and is reported in most sleep study results. On average, people with OSA experience a greater AHI during supine sleep (sleeping on the back) than nonsupine sleep, and during lighter sleep stages than deep slow-wave-sleep.38,39 The Figure shows average AHI in different sleep stages and in supine and nonsupine sleep in a sample of patients with at least moderate OSA who completed level 2 (home-based) polysomnography studies.38
{kind=link}
Differential diagnosis and comorbid sleep disorders
It is important to differentiate OSA from other disorders that can cause sleep fragmentation and result in similar daytime functional impairments. Central sleep apnoea is a sleep-related breathing disorder that results from reduced central drive to breathe rather than continued respiratory effort against a narrow or closed airway, and patients with this condition should be referred for management by a sleep specialist. Nocturnal hypoventilation refers to slow or shallow breathing during sleep. It can be associated with different medications or substances, such as narcotics, opioids, sedatives and alcohol, and is associated with other conditions such as obesity, chronic obstructive pulmonary disease, other respiratory diseases and neurological and musculoskeletal problems. Patients presenting with suspected narcolepsy, restless legs or periodic leg movements during sleep should also be referred for management by a sleep specialist. OSA can also overlap with other sleep disorders that require adjunctive therapy.18
Managing OSA in general practice
All people with OSA should be provided with education about OSA, risk factors, immediate symptoms and long-term consequences. OSA treatment considerations may be based on OSA severity (mild, moderate, severe), the presence of supine-predominant OSA (mainly present when sleeping on back), patient treatment preferences and lifestyle factors and the presence of comorbid sleep, mental and physical conditions.
Sleep specialist referral
An increase in the prevalence of OSA presentations in Australian primary care and reliance on specialist sleep services in Australia has resulted in long waiting lists and reduced capacity of the specialist services to manage patients with complex OSA or comorbid conditions.40,41
Several randomised controlled trials have compared models of sleep apnoea management in general practice versus specialist sleep centres.42-44 GP and practice-nurse management of sleep apnoea has similar effectiveness to management in specialist sleep centres.45 Referral to a sleep specialist is recommended for patients:
- with very severe OSA
- with excessive daytime sleepiness (e.g. score ≥16/24 on the Epworth Sleepiness Scale)
- with a history of motor-vehicle accidents or significant driving or occupational accident risk
- with other comorbid or complex conditions (e.g. central sleep apnoea, morbid obesity, alcohol misuse, chronic opioid use, heart failure, neuromuscular or chest wall deformity, uncontrolled psychiatric disorder, chronic obstructive pulmonary disease, requirement for supplemental oxygen, or other significant sleep, respiratory or cardiac disorders)
- who are commercial drivers
- in whom the cause of excessive sleepiness is unknown following a sleep study
- with poor treatment response (e.g. to CPAP or MAS).12
Mild and minimally symptomatic OSA
Patients with mild and minimally symptomatic OSA may respond to specific treatments that should be guided by presenting complaints and patient preferences. For example, compared with standard care, CPAP therapy is associated with improvement in sleepiness, fatigue, mental health and quality of life in patients with mild OSA (AHI, 5 to 15).46 Patients with mild OSA and a chief complaint of loud snoring may show an adequate response to an MAS. Among patients with mild OSA and no associated symptoms, GPs may consider management approaches based on the presenting symptoms and review and reassess for OSA over time.
CPAP therapy
The recommended first-line treatment for moderate and severe OSA is CPAP therapy combined with lifestyle and/or weight management advice.2,13 Following assessment and diagnosis of OSA, GPs may refer patients with OSA to a CPAP provider to access CPAP therapy. The cost of CPAP therapy is subsidised by some private insurance policies. People treated with CPAP wear nasal or oronasal interfaces that deliver positive pressure into the airway during sleep. At the required pressure level, CPAP prevents airway narrowing (hypopnoea) and closure (apnoea) events during sleep, resulting in stable oxygen saturations, elimination of sleep fragmentation caused by cortical arousals and improved daytime function in many patients.13
Although CPAP therapy is a very effective treatment, about half of patients find it difficult to accept CPAP initially, or discontinue CPAP use over time.14 Patients should be offered acute and ongoing support to identify and overcome any barriers that may cause poor adherence to CPAP therapy. Predictors of long-term adherence include early adherence and side effects, sleep apnoea severity, presence of daytime symptoms, psychological factors and comorbidities (e.g. insomnia).22,47,48 It is therefore important to ensure that patients are well educated about the benefits of CPAP therapy in relation to their OSA symptoms, and that early CPAP side effects are successfully addressed.49,50 Patients should be encouraged to use CPAP therapy regularly rather than intermittently. General sleep and sleep hygiene information is available from the Sleep Health Foundation (Box 2).12 Interventions that may improve adherence include education, behavioural therapy (motivational interviewing and cognitive behavioural therapy for insomnia symptoms), peer support and telehealth delivered to patients in individual, peer-to-peer or group format, troubleshooting and telemonitoring interventions.32,51-53 Some of these services may be accessed through psychologists or counsellors (for example, motivational interviewing, behavioural interventions) and CPAP providers (for identifying and overcoming problems with CPAP equipment). Patients who fulfil specific criteria may be eligible for government-subsidised CPAP equipment depending on the state or territory and local health network in which they reside (Box 2).
{kind=link}
Lifestyle, weight management and good sleep habits
Overweight/obesity is one of the strongest risk factors for OSA.12 Accordingly, all patients with overweight/obesity and OSA should be offered advice about reducing their body weight. Randomised controlled trial evidence indicates that lifestyle interventions including exercise, diet and combination interventions can reduce OSA severity.54,55 A meta-analysis of seven randomised controlled trials reported that weight loss intervention resulted in a significant AHI reduction (average reduction = 6.04 events per hour of sleep). Although statistically significant, this small AHI difference was not sufficient to reduce OSA severity to nonclinical levels in most patients.54
Patients with OSA should also be offered advice regarding reducing excessive alcohol consumption and, when possible, avoiding sedative-hypnotic medicines and other medicines that can contribute to next-day sleepiness.12 GPs are well placed to also provide advice about good sleep habits (e.g. maintaining a regular sleep/wake schedule, ensuring sufficient time in bed for sleep) and sleep hygiene (e.g. avoid watching television in bed and large meals immediately before bed) as well as cognitive behavioural therapy for insomnia (CBTi), or referral for CBTi, for comorbid insomnia symptoms.56
CBTi improves insomnia in the presence of OSA.24 It may improve subsequent management of OSA via increased CPAP adherence, as well as mental health symptoms.32,57 CBTi has historically been administered by trained therapists or psychologists over six to eight weekly sessions but has also been translated to self-guided reading materials and interactive online programs.58
Patients who are managed with lifestyle or weight management approaches as the only intervention should be reassessed every two to three months to identify any exacerbation of symptoms, comorbidities or change in work or lifestyle factors that may indicate reconsideration of the treatment approach. For example, additional treatment may be considered if the patient’s weight increases, if snoring becomes louder and more noticeable to a bed partner, or if daytime symptoms such as sleepiness, fatigue, lethargy or poor mood increase (Box 1).
Dental device – mandibular advancement splint
MASs, also known as oral appliance devices, are custom-fitted devices that can reduce OSA severity and snoring by moving the lower jaw and tongue forwards.59 Simple mouthguards purchased without dental guidance may damage the teeth and are often ineffective. Patients with OSA who do not wish to use or cannot tolerate CPAP therapy may be referred to certain dentists who offer ‘sleep’ services for consideration of MAS management of OSA.13,59 A patient fact sheet on MAS is available from the Sleep Health Foundation (Box 2).
Positional therapy
OSA severity is generally worse during supine sleep, compared with nonsupine sleep.38,39 This information is available in level 1 and 2 sleep study reports. Therefore, patients with supine-predominant OSA may be offered advice about positional therapy or a positional control device to reduce supine sleep and overall severity of their OSA.12,60 Positional therapy is recommended for patients with mild and moderate OSA, who have an AHI that is at least twice as high in supine versus nonsupine sleep and can tolerate sleeping in the nonsupine position. Importantly, a diagnostic test including a positional sensor is required to identify patients suitable for positional therapy. Many level 3 and 4 sleep study devices do not monitor sleeping position throughout the night and cannot be used to identify supine-predominant OSA. Positional therapy may also be used in combination with other therapies to promote greater AHI reduction.61
Surgery
Upper airway surgery may be considered for patients with significant craniofacial abnormalities (craniofacial surgeon) or mild OSA with a crowded upper airway, or those in whom CPAP and/or MAS therapy are not tolerated or effective (ear nose and throat specialist surgeon). A recent guideline reports on the efficacy of different surgical techniques in reducing OSA severity.12
Conclusion
OSA is a prevalent and debilitating condition that is frequently managed by Australian GPs. It is important they be aware of the large variability in presenting symptoms, standardised screening tools, sleep study referral options and evidence-based management approaches.
Translation of best practice management of OSA to general practice settings is the basis of our research group’s involvement in an NHMRC-funded program that aims to provide GPs with the tools, treatment and referral options to manage sleep disorders in general practice – the National Centre for Sleep Health Services Research (NCSHSR) program, Positioning Primary Care at the Centre of Sleep Health Management (2018-22). All GPs who are interested in becoming involved in this research program, in receiving research outputs or who want to contribute feedback about this article or experiences from your own practice are welcome to contact us via the NCSHSR email address (contact@ncshsr.com). RMT
COMPETING INTERESTS: All authors receive research grant funding and are provided with equipment for research from Philips Respironics and ResMed. Associate Professor Vakulin, Dr Lovato and Professor Adams are also provided with equipment for research by Sleeptite; they hold various institutional and professional leadership unsalaried roles. Professor Adams also receives research grant funding from The Hospital Research Foundation and the Freemasons Centre for Male Health and Wellbeing.