Untangling chronic breathlessness in primary care

Dr Sunjaya is a Scientia PhD Scholar in the Respiratory Group, George Institute for Global Health, UNSW Sydney; and Deputy Convenor of the Primary Care SIG, Thoracic Society of Australia and New Zealand. Ms Poulos is an Epidemiologist at the Australian Centre for Airways Disease Monitoring (ACAM), Woolcock Institute of Medical Research, The University of Sydney. Professor Reddel is an Honorary Visiting Medical Officer in the Department of Respiratory Medicine, Royal Prince Alfred Hospital, Sydney; and a Research Leader at the Woolcock Institute of Medical Research, The University of Sydney. Professor Jenkins is Head of the Respiratory Group, George Institute for Global Health; Professor of Respiratory Medicine at UNSW Sydney; Clinical Professor at Concord Clinical School, The University of Sydney, Sydney, NSW; and Chair of Lung Foundation Australia.
Breathing problems
Asthma
Chronic breathlessness is a common diagnostic and management challenge in daily practice. Although it is often associated with respiratory or cardiac conditions such as chronic obstructive pulmonary disease (COPD) and heart failure, several less common and systemic causes are important differential diagnoses not to be missed in daily practice.
- More than 9% of Australian adults report breathlessness; clinically important breathlessness is associated with poor quality of life, depression and anxiety.
- In most patients with chronic breathlessness, a systematic history and physical examination will guide the need for diagnostic investigations to rule out differential diagnoses or confirm a working diagnosis.
- A systematic approach to diagnosis can start with easily performed, noninvasive tests, which lead to a diagnosis in around 70% of people.
- If this approach does not result in a diagnosis and clear treatment approach, specialist referral should be considered.
Case scenario
Denise is a 37-year-old teacher who presents with breathlessness that has been troubling her over the past three years. She was diagnosed with asthma at the age of 3 years when she experienced wheezing with a cold. She gained relief from salbutamol administered with a spacer but never took a regular asthma preventive. At school, she sometimes took salbutamol before exercise or after a vigorous netball game when she felt chest tightness. She had allergic rhinitis triggered by exposure to cats and house dust. She occasionally had chest tightness with colds, which was sometimes but not always helped by salbutamol. During her 20s and early 30s, she was not troubled by asthma symptoms and took no medications.
Over the past three to four years, Denise’s breathlessness has recurred, not clearly related to allergic triggers. She began to experience exertional dyspnoea when physically active, and felt she needed to slow down to prevent it worsening. She changed her swimming stroke from freestyle to breaststroke to help her control her breathing more effectively. Nevertheless, she has excellent exercise capacity in certain circumstances, and is able to do 10 km in 30 minutes on a stationary bicycle and to talk easily while walking laps of a large local park with friends.
Commentary
Impact of breathlessness on patients
A recent study of 10,072 randomly sampled adults in Australia found that 9.5% have breathlessness.1 This National Breathlessness Survey found that clinically important breathlessness (a score on the modified Medical Research Council dyspnoea scale of 2 or above) was associated with poor quality of life and depression and anxiety.1 Of concern, half of the people who reported clinically important breathlessness did not report a diagnosis of a respiratory or heart condition, suggesting either that breathlessness is caused by other conditions or that respiratory or heart conditions are being underdiagnosed in Australia.1 Either way, the findings highlight the need for thorough investigations of breathlessness in primary care before commencing empiric treatment.
Distinguishing respiratory, cardiac and systemic causes of breathlessness
In most cases, cardiac or respiratory causes of breathlessness can be identified by careful history taking, even though accurate diagnosis (such as determining whether the diagnosis is asthma rather than chronic obstructive pulmonary disease [COPD] in an older ex-smoking patient) will require further testing. A study of 123 patients with chronic breathlessness found that only 55% of physicians’ predictions made after history taking and examination were accurate, when compared with the final diagnoses.2
Patients with chronic breathlessness often present during an acute exacerbation. Before detailed further examination, red flags can indicate a requirement for urgent referral. Critical acute features include central chest pain, stridor or marked breathing effort with fatigue, new confusion or increased drowsiness (observed or reported), signs of hypoxaemia and massive haemoptysis. Subacute features of concern that necessitate urgent referral include persistent cough (lasting more than three weeks), weight loss or fever.3,4
History taking
Key questions to consider for assessing breathlessness are as follows.
- Clarify key aspects first. Ascertain if this is definitely shortness of breath. Could the patient be experiencing fatigue? Is there associated leg discomfort, progressive loss of energy, weakness or any other general features not specific to breathing?
- Age of onset. At what age did this first occur? Has it been variable? Has there been any symptom-free interval (weeks, months or years)? Were similar symptoms present in childhood?
- Setting. Does it occur only in particular settings – at work, at night, standing up or lying down, when anxious or stressed, during activities, with hobbies? Does it improve on holidays or weekends?
- Risk factors. Ask about family history, smoking history, occupational history (consider possible interstitial lung diseases such as silicosis, asbestosis), current medications and comorbidities, and past diagnoses.
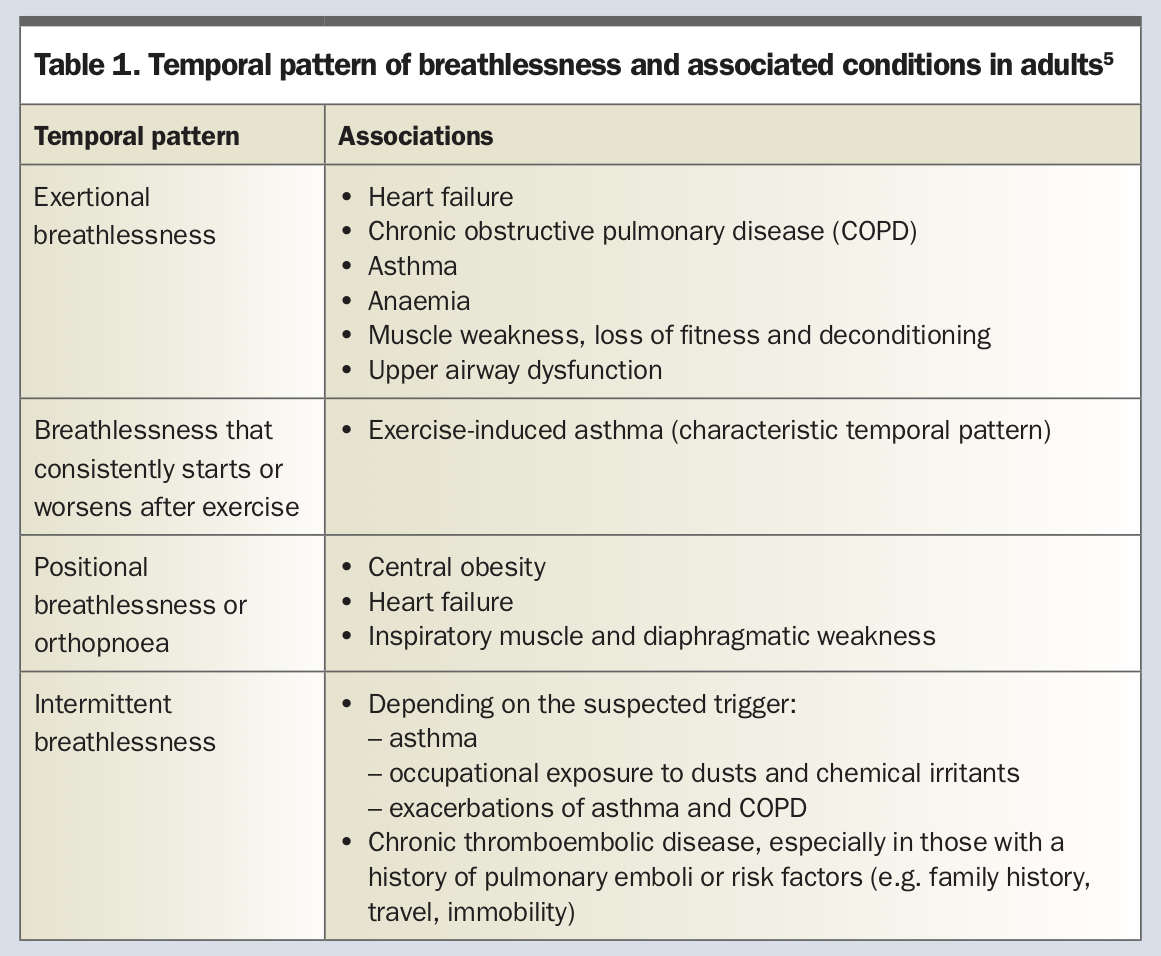
- Timing. When does it occur, what triggers it, how long does it last, what relieves it? Does it occur at rest? If only on exertion, when does it commence and how long does it last after exertion ceases? The temporal patterns of breathlessness and associated conditions in adults are shown in Table 1.5
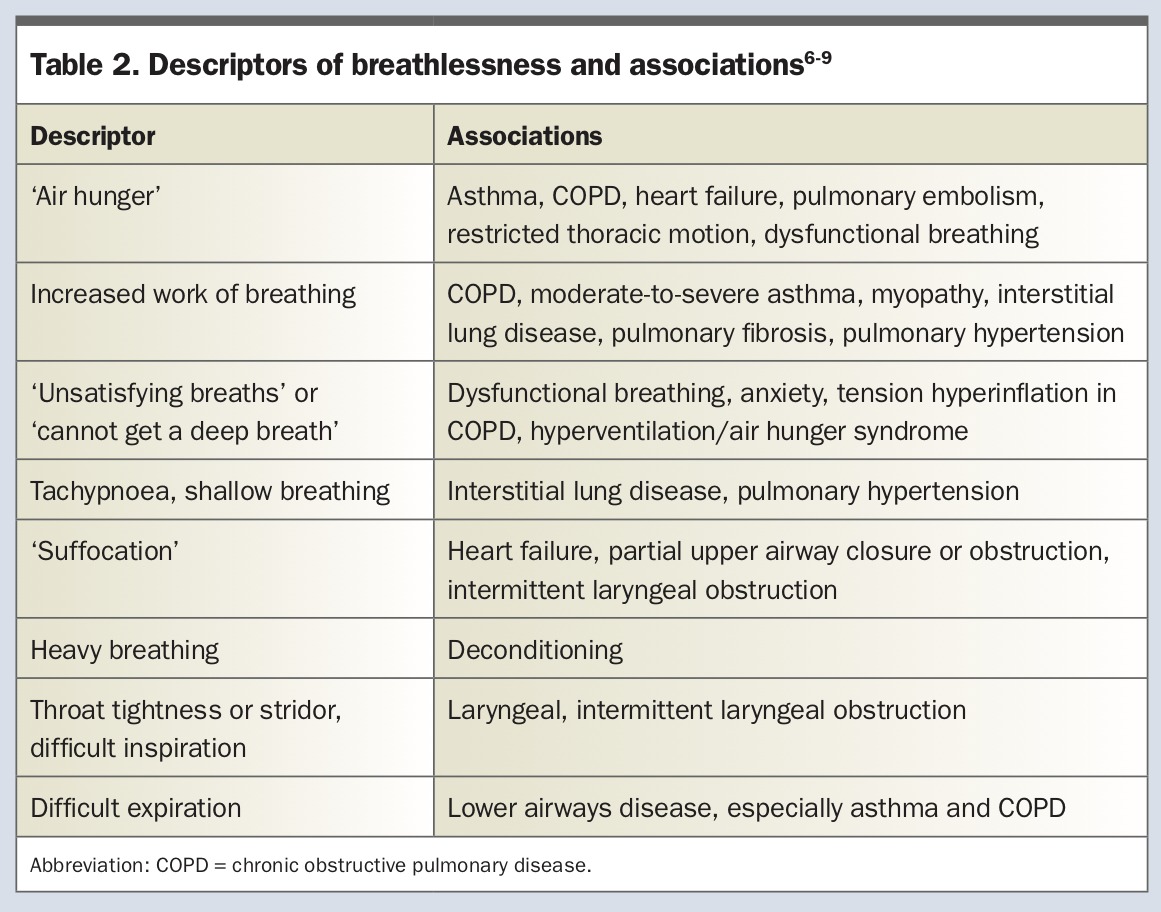
- Features. Describe the sensation – is it fast breathing, shallow breathing, laboured or difficult breathing? Chest heaviness or tightness? Or is it a sensation of inability to breathe deeply enough? Ask the patient to point to where they feel the sensation. Descriptors of breathlessness and their associations are shown in Table 2.6-9
- Associated features. What other features are present (e.g. wheeze, stridor, cough, chest pain, light-headedness, anxiety or apprehension)? Understand that shortness of breath is very worrying and can trigger anxiety.
– Cough: ascertain whether dry or productive, repetitive, occurs singly or in bursts or paroxysms, sputum colour, origin and location (chest or throat and upper airway), what starts and relieves it, timing (night, day) and frequency
– Wheeze: confirm whether expiratory, intermittent or persistent
– Stridor: confirm that this is inspiratory, ask patient to point to location (usually laryngeal), ask about hoarseness and dysphonia to confirm laryngeal origin
– Chest pain: ask all cardiac questions, including relation to exertion, rest and relief, location and radiation, characteristics (sharp, crushing, dull ache), any associated symptoms of sweating, nausea, palpitations, light-headedness, sense of dread
– Chest tightness and dyspnoea on exertion: this may be associated with pulmonary hypertension, hypertrophic obstructive cardiomyopathy, congenital valvular disease or coarctation of the aorta
– Anxiety: ask about any specific triggers or settings, any associated symptoms to suggest a panic attack
– Additional systemic features: ask about ankle swelling, abdominal swelling, fatigue, weight gain or loss, mood, sleep quality, snoring, nasal obstruction, activities of daily living, physical activity on most days, symptoms of anaemia and possible causes (e.g. chronic gastrointestinal blood loss, heavy menstrual bleeding, iron deficiency due to poor intake and comorbidities).
{kind=link}
{kind=link}
Breathing SPACE approach
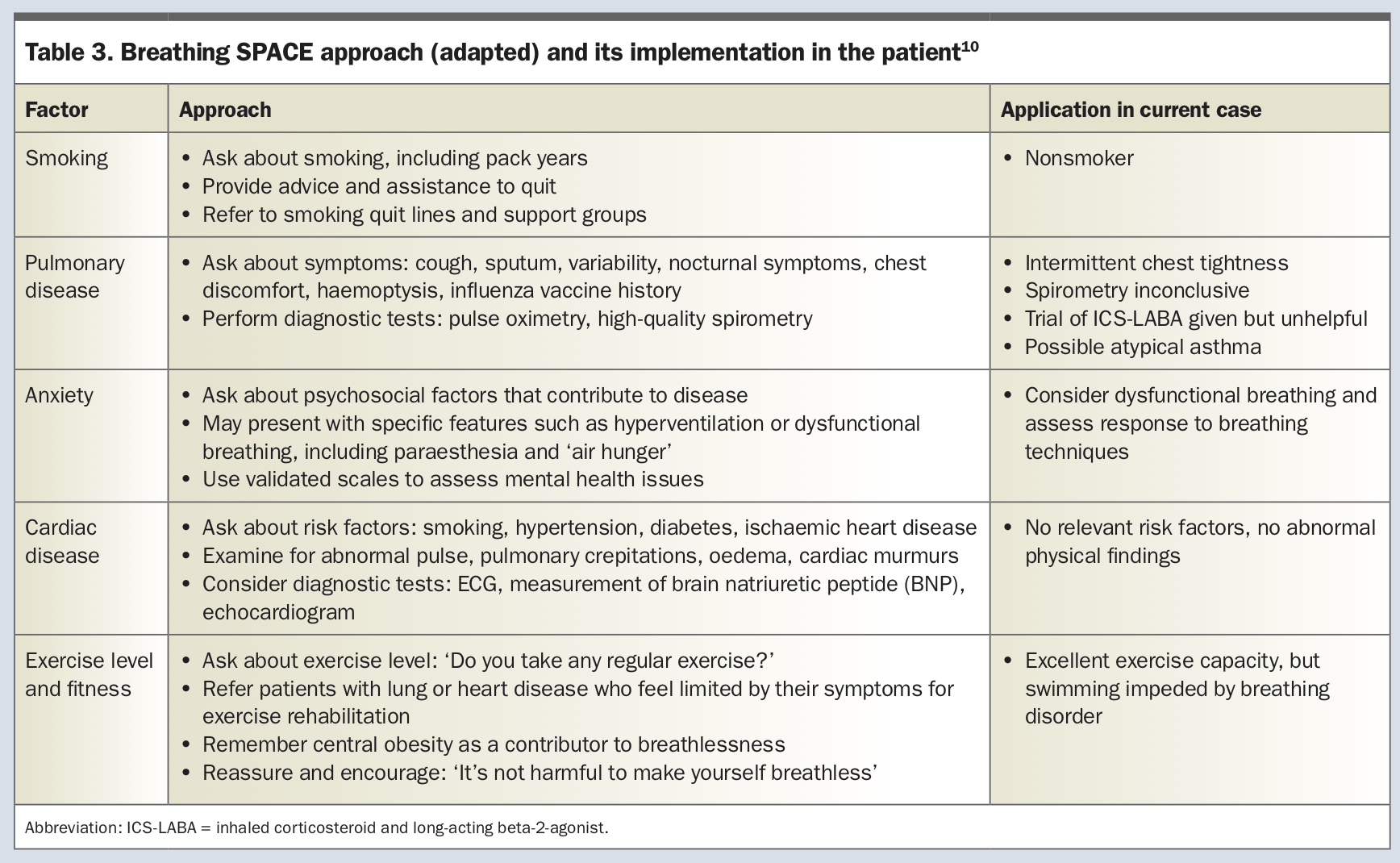
Acknowledging the multifactorial and multimorbid nature of breathlessness, the London Respiratory Network has developed a simple tool called Breathing SPACE, to support a systematic assessment of those with breathlessness.10 This tool focuses on enquiring about smoking, pulmonary disease, anxiety (and relevant psychological disorders), cardiac disease and exercise level or fitness, and relevant investigations and interventions. Details and their application to Denise are summarised in Table 3.10 Breathing SPACE questions can be quickly implemented in practice.
{kind=link}
Physical examination
The physical examination is also important, even though there may be no signs at rest when breathlessness is primarily exertional.
- Respiratory rate at rest should be measured as it may be elevated in people with early interstitial lung disease, upper airway obstruction, airway compression, significant pleural effusion, lobar collapse or anxiety.
- The patient should be asked to cough, which can reveal an upper or lower airways origin as well as the presence of secretions.
- The oropharynx should be examined for local masses and any signs of obstructive sleep apnoea.
- Signs of anaemia should be sought including pallor in the conjunctiva and palms.
- Chest examination should include listening over the trachea, assessment for accessory muscle use, tracheal location or tug and chest expansion. It is essential to listen for breath sounds, their distribution right and left, upper to lower zones, adventitious and airway sounds, during near to full inspiration and expiration as well as quiet breathing. Percussion should reveal dullness if a significant effusion or consolidation is present.
- Cardiac examination may reveal crucial signs and is an essential part of initial assessment for chronic breathlessness, even when an ECG is planned as the next step. Heart rate and rhythm, pulse volume and the pattern of any irregularity, the presence of peripheral oedema and its extent, raised jugular venous pressure, precordial lift, thrills and apical location and features may point to the underlying cause. The presence of a murmur and associated gallop or extra sounds can further help identify a likely cause for breathlessness if underlying cardiac abnormalities are detected.
Although many signs will be confirmed by imaging, a careful examination will help rule in or out some important diagnoses and help prioritise investigations. Beyond this, several validated practical questionnaires can aid clinical assessment, including the PHQ-9 for depression, GAD-7 for anxiety, DASS-21 for depression, anxiety and stress or K10 for psychological distress.11-15 Validated breathlessness severity scores such as the Borg Scale, visual analogue scale (VAS), Dyspnoea-12 and others are also recommended to support severity tracking over time.16 Some disease-specific questionnaires are useful to assess symptom burden and treatment response after a diagnosis is made, such as the Asthma Control Questionnaire (ACQ-5) and the COPD Assessment Test (CAT).
High-yield investigations accessible in primary care
In most cases, a systematic history and physical examination will guide the need to conduct diagnostic investigations to either rule out a differential diagnosis or confirm a working diagnosis.
Spirometry
When lung disease is suspected, high-quality spirometry is of particular importance. Spirometry added to history and physical examination has been found to have a 72% accuracy for diagnosing the cause of breathlessness.2
In Denise’s case, when she first experienced exertional symptoms three years earlier, her spirometry results were normal. She was told that her symptoms were probably caused by dysfunctional breathing. She did not agree nor respond positively to the suggestion that her symptoms might be provoked by anxiety, overbreathing and stress. Just before the current review, her GP started a trial of fluticasone-formoterol 125 mcg/5 mcg once or twice daily, but so far this has not been helpful.
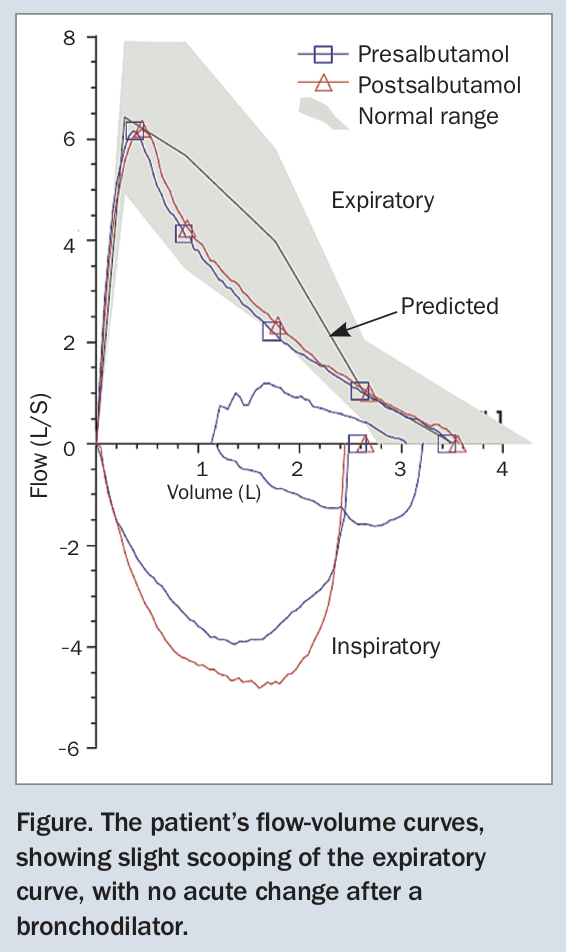
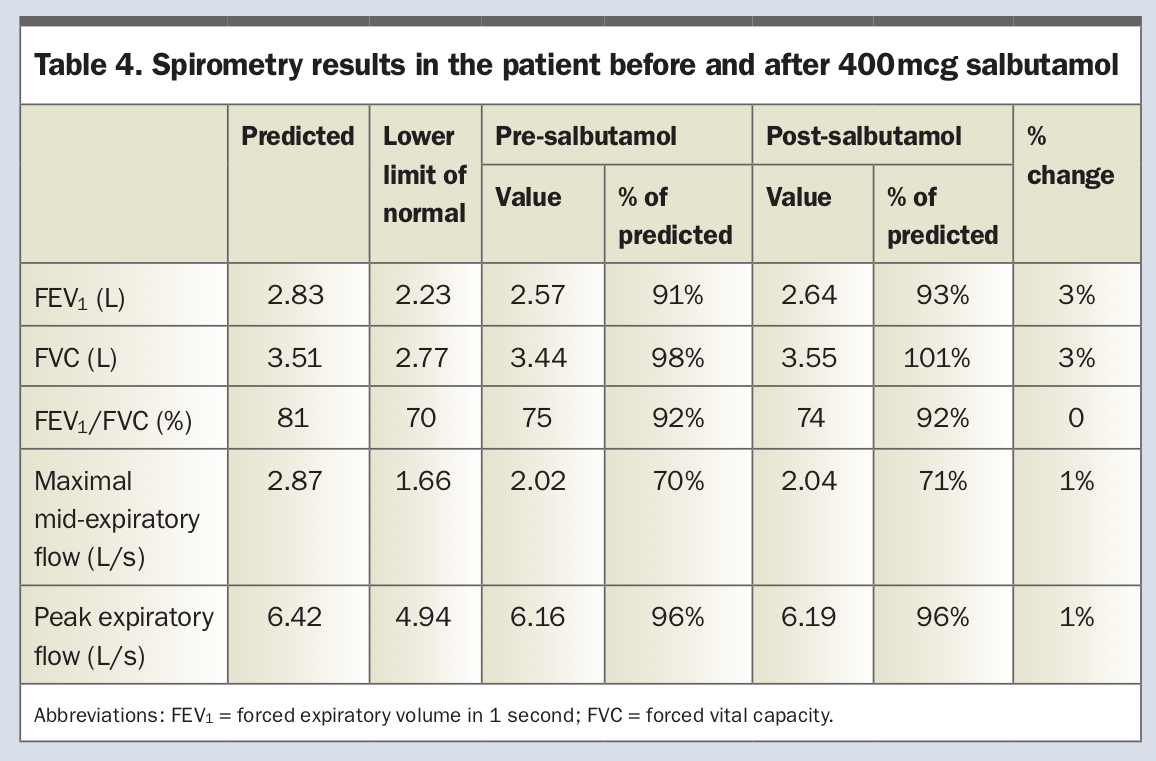
Denise’s current spirometry results after withholding her morning dose of inhaled medication show normal lung function (Figure and Table 4). Her forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) are 2.57 L and 3.44 L, respectively, or 91% and 98% of predicted. This gives an FEV1/FVC ratio of 0.75, with no change after 400 mcg salbutamol. Her expiratory flow-volume curve is slightly scooped, suggesting mild mid-flow obstruction, but within the normal range (Figure).
{kind=link}
{kind=link}
Other useful investigations
Other initial high-yield diagnostic tests commonly accessible in primary care are:
- pathology tests, specifically complete blood count, thyroid function tests and measurement of brain natriurietic protein (BNP)
- chest x-ray
- ECG.
Other tests that are useful but may require specialist referral include full lung volumes, diffusing capacity for carbon monoxide (DLCO) tests and echocardiography. For confirmatory diagnosis of deconditioning, patients can be referred for cardiopulmonary exercise testing (CPET). CPET enables a functional assessment of the cardiovascular, pulmonary and skeletal muscle contribution to exercise limitation and is especially useful to elucidate the cause of unexplained chronic breathlessness.
Update on Denise
Denise’s current symptoms are not typical of asthma and differ from her childhood symptoms. Asthma is not conclusively excluded by normal spirometry results while she is taking a combined inhaled corticosteroid (ICS) and long-acting beta-2 agonist (LABA), so this possibility should be reviewed after she ceases the ICS-LABA.
Denise is advised to slowly reduce her ICS-LABA to zero over a month and is then booked for a bronchial provocation test in a respiratory function laboratory after a further month. She is advised to use her short-acting beta-2-agonist (SABA) as needed for symptom relief in the meantime until she has the bronchial provocation test. She is given information and encouraged to try some breathing techniques and relaxation when she experiences symptoms.
Denise’s breathlessness is unchanged after she ceases the ICS-LABA. Her subsequent bronchial challenge test does not show airway hyper-responsiveness, and her spirometry results remain normal, suggesting asthma is not the explanation for her breathlessness. Rather, she finds breathing techniques helpful and notes an improvement in her symptoms despite having ceased the ICS-LABA.
To be more confident that there is no cardiac contribution to her dyspnoea, Denise has an ECG and echocardiogram, both of which show no abnormalities. Her lung volumes and diffusing capacity, measured at the time of initial spirometry, are also normal, indicating she does not have interstitial lung disease; and the normal diffusing capacity makes pulmonary vascular disease unlikely.
If breathing techniques were not helpful, particularly if Denise’s symptoms were associated with stridor or dysphonia, then referral to a speech pathologist and specialised voice clinic might prove useful to confirm intermittent laryngeal obstruction and help with laryngeal hygiene and relaxation.17,18 RMT
COMPETING INTERESTS: Dr Sunjaya: None. Ms Poulos has received research grants from AstraZeneca, GlaxoSmithKline and Novartis. Professor Reddel has received research grants from AstraZeneca, GlaxoSmithKline and Novartis, and payment for providing independent medical advice from Novartis, and independent medical education from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Sanofi and Teva; and sits on the advisory boards of AstraZeneca, Chiesi, GlaxoSmithKline, Novartis and Sanofi. Professor Jenkins has received a research grant from GlaxoSmithKline, payment for developing or providing independent medical education from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Novartis, and expert testimony from AstraZeneca and Novartis; and sits on the advisory boards of AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis and Sanofi.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.