Inhaled corticosteroids in COPD: when are they needed, when not needed and when harmful?


Professor Frith is Professor in Respiratory Medicine at the College of Medicine and Public Health, Flinders University, Adelaide; and Adjunct Professor in Health Sciences at the Alliance for Research in Exercise, Nutrition and Activity (ARENA), University of South Australia, Adelaide, SA. Professor Yang is Head of the Northside Clinical School, The University of Queensland; and Thoracic Program Medical Director at The Prince Charles Hospital, Brisbane, Qld. Dr Hancock is a GP Principal at Chandlers Hill Surgery, Adelaide, SA; an Executive Member of the COPD Coordinating Committee of Lung Foundation Australia (LFA); Chair of the GP Advisory Committee, LFA; and C hair of the Respiratory Medicine N etwork, Specific Interests Faculty, RACGP.
COPD (chronic obstructive pulmonary disease)
Breathing problems
Inhaled corticosteroids (ICS) have revolutionised asthma control but have a lesser role in patients with chronic obstructive pulmonary disease (COPD) and no asthma. ICS increase risk of pneumonia and other risks in patients with COPD, and long-acting bronchodilators are just as effective in many. Nevertheless, some subgroups may benefit from ICS.
- Inhaled corticosteroids (ICS) have revolutionised asthma control, but their use in patients with chronic obstructive pulmonary disease (COPD) is not as definitive.
- Long-acting bronchodilators help control symptoms and reduce the risk of exacerbations for most patients with COPD.
- Adding ICS to dual long-acting bronchodilators reduces exacerbations in patients with a history of recurrent exacerbations or coexisting asthma, especially if blood eosinophil counts are high (more than 0.35 x 109 cells/L).
- However, use of ICS by patients with COPD increases the risk of pneumonia and some metabolic consequences.
- ICS should not be used in patients with mild-to-moderate COPD; if already prescribed in these patients they can be judiciously withdrawn.
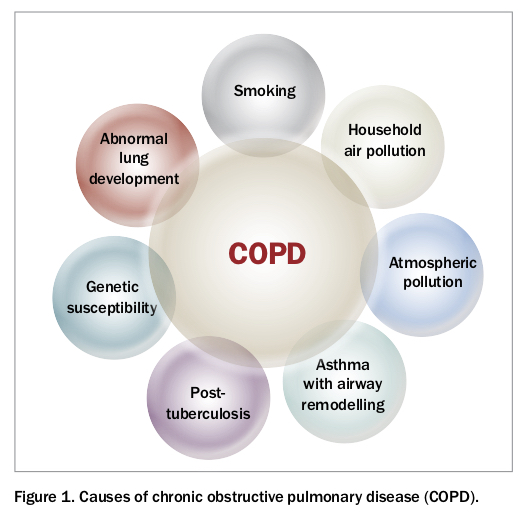
Chronic obstructive pulmonary disease (COPD) is a common and disabling chronic condition, affecting about 10% of the Australian population aged over 40 years, and the third highest cause of disablement from noncommunicable diseases worldwide.1 Although the most common cause of COPD in Australia is cigarette smoking, from a global perspective household air pollution and atmospheric pollution account for at least as much disease as smoking.1-3 Asthma, bronchiectasis and tuberculosis are other important causes (Figure 1).3
{kind=link}
In the past, COPD was considered essentially untreatable. However, the development of new therapies and guidelines on their use now allows us to treat patients with COPD. Our understanding of how to use modern medications has been so refined that we can begin to apply treatments according to the clinical characteristics or phenotype of the individual patient with COPD – so called personalised care or ‘treating traits’. This article discusses an aspect of this approach, focusing on the use of inhaled corticosteroids (ICS) to treat patients with COPD.
Challenges of treating COPD
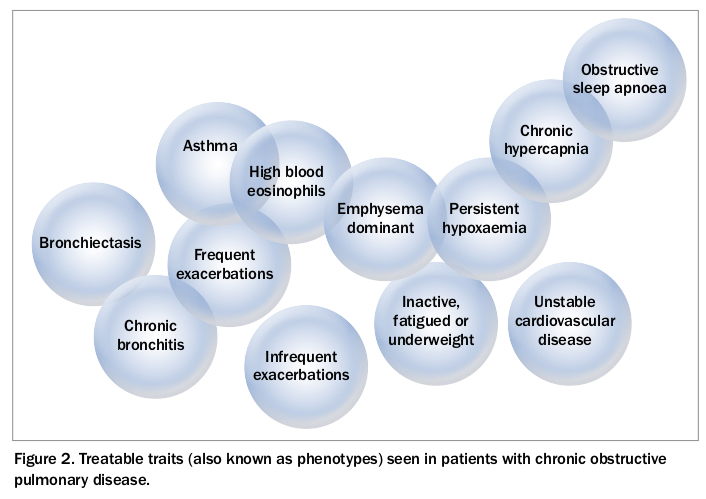
Depending in part on the aetiology of COPD, its main characteristics range between airway remodelling with fixed airflow limitation, dropout of functioning airways, partially reversible mainly small airways obstruction, luminal airway blockage by secretions and emphysema.3 The defining characteristic is airflow limitation, so the definition requires demonstration of airflow limitation with spirometry. The globally standardised criterion is a ratio of forced expiratory volume in one second (FEV1) to forced vital capacity (FVC) below 0.7. Usually, this is accompanied by a reduced FEV1 (80% of the predicted normal value).2,3 The clinical manifestations of COPD cover a wide range, often referred to as phenotypes or treatable traits (Figure 2).4 Many studies have tried to identify meaningful endotypes of COPD (characterised by specific cells or molecules in blood or sputum), and recent research suggests the excess or paucity of eosinophils in blood may prove clinically useful.
{kind=link}
All these features add to the complexity of COPD, a condition that until recently was considered inexorably progressive, ultimately fatal and essentially untreatable. Small wonder that little interest was taken in COPD in the past, and efforts to improve diagnosis and develop new treatments were often wasted.
Changed understanding of COPD management
Since the late 20th century there have been progressive reductions in smoking rates and the development of new drugs to treat COPD, with improved efficacy and tolerability and more effective delivery systems. Trials evaluating how the pharmacological and nondrug treatments that are now available work best in combinations, and the emergence of powerful statistical analyses such as systematic reviews and meta-analyses have all contributed to the development of guiding documents on COPD. These include expert consensus statements, evidence-based recommendations, guidelines and toolkits. We have substantially changed our understanding of and empathy with patients with COPD and our interest in helping them manage their disease.
Twenty years ago, there was little interest in varying treatment of airways diseases from the recommended treatments for asthma. In the 1990s, new guidelines for diagnosis and treatment of COPD were developed, based on new research involving both old and new drugs as well as pulmonary rehabilitation. These guidelines included the evolving Australian and New Zealand guidelines for the management of COPD (the COPD-X plan) and the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Report initiated in 2001.2,3,5,6
Why, or why not, consider inhaled corticosteroids?
ICS have cemented their position as the single most important drug treatment for asthma, and correct use of ICS in that setting has contributed greatly to reducing hospitalisations and deaths from asthma over the past 30 years.7,8 ICS are most effective in patients with eosinophil-based inflammation (the predominant pattern in asthma).
On the other hand, in COPD neutrophils drive the predominant inflammatory pathways, and eosinophilic inflammation is uncommon, making the routine use of ICS unnecessary. However, when ICS are used with inhaled long-acting beta-2 agonists (LABAs), extensive reports have shown better lung function and quality of life and fewer exacerbations in people who have had previous exacerbations and more severe airflow limitation, summarised in the COPD-X plan.6,9
In the past 10 years, it has also become clear that use of ICS in patients with COPD contributes to increased risk of pneumonia, tuberculosis and non-tuberculous mycobacterial infections.9,10 Other potential important adverse consequences include oropharyngeal side effects, diabetes mellitus, low bone mineral density and cataracts.11-14 Limiting the use of ICS to specific settings is therefore now advisable.
Curiously, ICS use has not been associated with pneumonia in patients with asthma, although this may be explained by different patterns of inflammation and an altered microbiome in COPD. Moreover, information from large trials in patients with COPD has begun to show that low eosinophil levels predict a higher likelihood of pneumonia, sepsis and worse outcomes from exacerbations in patients who are receiving ICS.15,16
In Australia, the COPD-X guidelines recommend use of ICS (as part of combination inhalers) for COPD only for patients with severe symptomatic COPD and FEV1 less than 50% predicted who also have frequent exacerbations.2 ICS are subsidised by the PBS only for this patient group, now as a ‘streamlined authority’ for ICS-LABA or ICS-LABA-LAMA (inhaled long-acting muscarinic antagonist) combinations.
Although definitions of ‘frequent exacerbations’ vary, GOLD suggests that they be defined as:
- one or more severe exacerbations in a year requiring hospitalisation, or
- two or more moderate exacerbations requiring oral corticosteroid and/or antibiotic therapy in the past year.3
What evidence supports ICS for patients with frequent exacerbations?
Exacerbations are events that are associated with an escalation of respiratory symptoms requiring added therapies (or even hospitalisation) to control.3 They are experienced by many patients with COPD and have major consequences, with prolonged diminution of quality of life through heightened breathing difficulties, cough and other symptoms.17,18 In addition, 12-month mortality rates after a severe exacerbation of COPD (requiring hospitalisation) are higher than after myocardial infarction.3
Given the impact of exacerbations, one of the two central goals of COPD treatment is to reduce the risk of exacerbations by identifying characteristics of patients that predict that risk. The leading predictor is a previous history of exacerbations.3,19 There are recent suggestions that the risk may be even better predicted by a combination of historical exacerbations and blood eosinophil counts, although convincing evidence of this is not available.
Randomised controlled trials of ICS in COPD have been conducted over the past 20 years.20,21 They have resulted in many editorials, systematic reviews and meta-analyses. These reports have been enhanced by two recent large trials and a systematic review, which showed that the risk of exacerbations reduces with ICS use compared with both placebo and LABA use.22-24 A recent study also shows that adding an ICS to therapy for patients hospitalised for an exacerbation may reduce subsequent exacerbations.25
How can we predict which patients should take an ICS?
However, prospective trials are still needed to determine the usefulness of this score in guiding ICS use.
Meanwhile, as a personal perspective, we suggest two new algorithms to guide initial treatment choices and follow-up treatments, respectively (Flowchart 1 and Flowchart 2). These are based on trials and meta-analyses that address individual and comparative efficacy and effectiveness of ICS, as well as their safety, together with trials reporting beneficial and potentially harmful effects of corticosteroid withdrawal or replacement. These algorithms are suggestions only, as the area remains controversial, especially in relation to the role of blood eosinophil levels in driving treatment decisions.
Other algorithms, with varying grades of complexity, have been presented in peer-reviewed and evidence-based publications from national and international organisations, but only the COPD-X is applicable to Australian PBS prescribing.3,27,28 Evidence is mounting that lower doses of ICS may be preferable.
What should I do if my patient is taking an ICS that I think is not necessary or advisable?
It is common to find patients with COPD who have been prescribed ICS when in fact they do not need them. Overuse of ICS has been documented in most countries, and ICS have often been prescribed as initial treatment.29 The COPD-X plan recommends that GPs and specialists review patients with COPD regularly, according to the severity of their disease symptoms or when they have had an exacerbation. If a patient has evidence of adverse corticosteroid effects (e.g. recent pneumonia, osteoporotic fractures, poorly controlled diabetes, troublesome oral candidiasis, hoarse voice) and if the patient characteristics do not meet ICS indications then the ICS can now be confidently withdrawn, based on a number of trials.30-33
Conclusion
COPD is a complex chronic disease, with many multimorbidities and a complicated clinical trajectory. Fortunately, management options are continually evolving, with both nonpharmacological and pharmacological therapies now available to further help our patients. Some take-home messages about ICS use in patients with COPD are listed in the Box.
{kind=link}
In summary, regarding use of ICS in patients with COPD:
- When are ICS needed? In patients with COPD who have coexisting asthma or severe airflow obstruction (FEV1 less than 50% predicted) with frequent exacerbations, consider treatment with ICS in the form of an ICS-LABA combination plus a LAMA or a ICS-LABA-LAMA combination.
- When are ICS not needed? Patients with mild-to-moderate COPD do not require ICS. Instead, use long-acting bronchodilators (a LAMA, a LABA or a LAMA-LABA combination).
- When are ICS harmful? In patients with adverse effects, such as pneumonia or metabolic or other effects, consider withdrawing ICS. RMT