Influenza vaccination – important at all ages

Dr Li-Kim-Moy is a Clinical Research Fellow at the National Centre for Immunisation Research and Surveillance and the Children’s Hospital at Westmead, Sydney; an Honorary Research Fellow at The University of Sydney; and a General Paediatrician in Sydney. Professor Macartney is the Director of the National Centre for Immunisation Research and Surveillance, Sydney; a Paediatric Infectious Disease Consultant at the Children’s Hospital at Westmead, Sydney; and Professor in the Discipline of Paediatrics and Child Health at The University of Sydney, Sydney, NSW.
Influenza
Immunisation
Influenza continues to cause a substantial burden on the community. Widening recommendations, a focus on vaccinating children, improved access to funded vaccination and new enhanced vaccines for older adults are all aimed at improving control of influenza.
- Influenza is increasingly recognised as being responsible for a large burden of disease not only in older people and people with medical conditions that increase the risk of severe influenza, but also in healthy young children, pregnant women and Indigenous Australians.
- Vaccination provides good protection and is recommended for all people from 6 months of age.
- Age-appropriate vaccines should be used in children; enhanced vaccines, which induce a stronger immune response, are preferentially recommended for people aged 65 years and over.
- Free vaccination under the National Immunisation Program is available for older adults, people with certain comorbid conditions, pregnant women and all Aboriginal and Torres Strait Islander people. State-funded programs provide free vaccine for children aged from 6 months to under 5 years of age.
Influenza is a common viral respiratory infection that causes a large burden of disease globally, through annual (typically winter season) epidemics. It is the most common vaccine-preventable disease in Australia.1 Although it is of mild-to-moderate severity in most people, severe disease can occur in previously healthy people of any age, but especially older people and those with comorbidities. Worldwide, influenza is estimated to cause three to five million cases of severe illness and about 290,000 to 650,000 respiratory deaths each year.2
Influenza epidemiology in Australia
Influenza has the greatest impact on the community at the extremes of age – the young and older people – as well as among those with medical comorbidities. Documented hospitalisation and mortality rates underestimate the true disease burden of influenza, in part owing to incomplete recognition of disease, undertesting and late complications of infection (such as bacterial pneumonia or myocardial infarction).
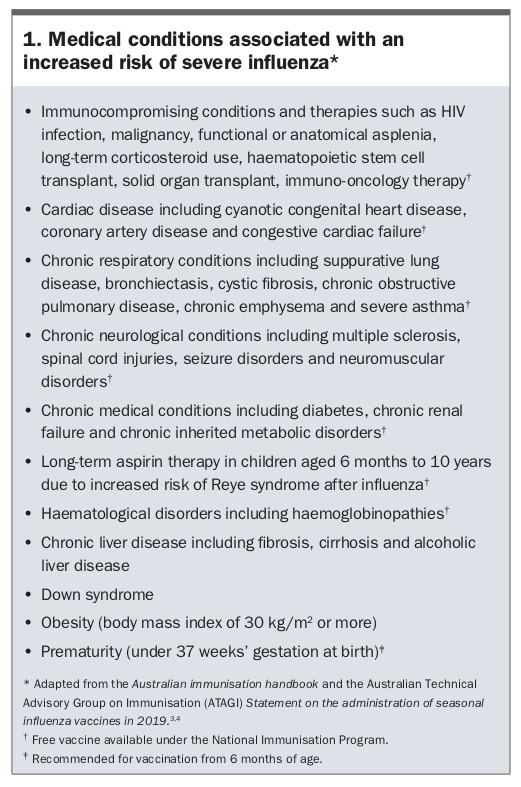
Because of immunosenescence and an increased prevalence of comorbid conditions associated with severe influenza, older people have increased mortality and morbidity from influenza (Box 1).3,4 Less well known is the high burden of disease among other groups, such as children younger than 5 years who are often otherwise healthy. Young children have similar or higher hospitalisation rates due to influenza than older adults (108 to 187 per 100,000 in those aged under 2 years compared with 48 per 100,000 in those aged 75 years and over).5 Infection attack rates in the unvaccinated community are highest among children, estimated at 15 to 22.5% annually, and infected children are significant in the spread of influenza to the rest of the community.6-9 The incidence of influenza among babies under 6 months, who are too young to be vaccinated, is substantial. 5 They benefit from maternal vaccination during pregnancy, which results in transplacental transfer of high levels of influenza-specific antibody.10
{kind=link}
Pregnant women are at risk of more severe infection and have higher rates of intensive care unit admission.11 Influenza during pregnancy may be associated with increased rates of premature birth, fetal death and low birth weight.11 Evidence that vaccinating pregnant women protects their babies from influenza in the first 6 months of life can help guide decision-making for expectant mothers.10
Compared with the non-Indigenous population, influenza infection rates are 1.5 to 8.6 times higher among Indigenous Australians, depending on age, and Indigenous Australians of all ages are advised to receive annual influenza vaccination.5,12
Influenza vaccine strains and manufacture
Influenza vaccination is recognised as the most effective way of reducing influenza disease burden in the community. Vaccine effectiveness (VE; the proportionate reduction in infection among vaccinated people compared with nonvaccinated people) is moderate, typically around 40 to 60% in adults.13,14 However, this still means that vaccination reduces the risk of developing influenza by half and offers the best protection possible.
Circulating influenza strains continually change, and this is one of the main reasons, along with the relatively short duration of protection of influenza vaccines, why annual vaccination is recommended. Each year, the WHO recommends in February which influenza virus strains are to be included in the northern hemisphere vaccines, and in September makes a recommendation for the subsequent southern hemisphere seasonal influenza vaccines.15 Manufacturing (predominantly from egg-propagated virus) and testing of the influenza vaccines takes several months, and the southern hemisphere vaccines are usually available around March or April of the following year.
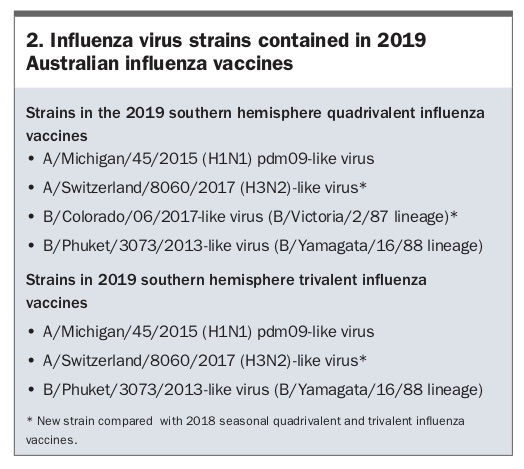
Quadrivalent influenza vaccines (QIV) have largely replaced trivalent influenza vaccines (TIV) as standard-dose vaccines (containing 15mcg influenza haemagglutinin for each virus strain per 0.5mL vaccine). Only enhanced influenza vaccines (see below) are currently trivalent. QIVs incorporate one influenza A subtype H1N1 virus, one influenza A subtype H3N2 virus, and two influenza B viruses, one each from the Yamagata and Victoria lineages (see Box 2 for 2019 influenza vaccine strains). The closeness of matching of vaccine and future circulating virus strains can vary, given the possibility of circulating virus mutations, and is an important factor in how effective the vaccine will be in any season.
{kind=link}
In 2017, Australia experienced a particularly severe influenza season with 251,150 laboratory-confirmed influenza notifications nationally, two-and-a-half times the previous record for annual notifications.1 That year was an influenza A(H3N2)-predominant year, typically associated with more severe disease in older people. The situation was also compounded by low VE of only 10% against influenza A(H3N2) strains, although VE for influenza A(H1N1) was 50% and VE for influenza B strains was 57%.16 The poor VE for influenza A(H3N2) may have been partly caused by recent A(H3N2) vaccine viruses propagated in eggs undergoing egg-adaptation mutations during manufacture, which in turn gives rise to antibodies after vaccination that are less effective against circulating viruses.17 Cell-derived or recombinant vaccines may solve this problem in the future.
Types of influenza vaccine
Standard-dose influenza vaccines
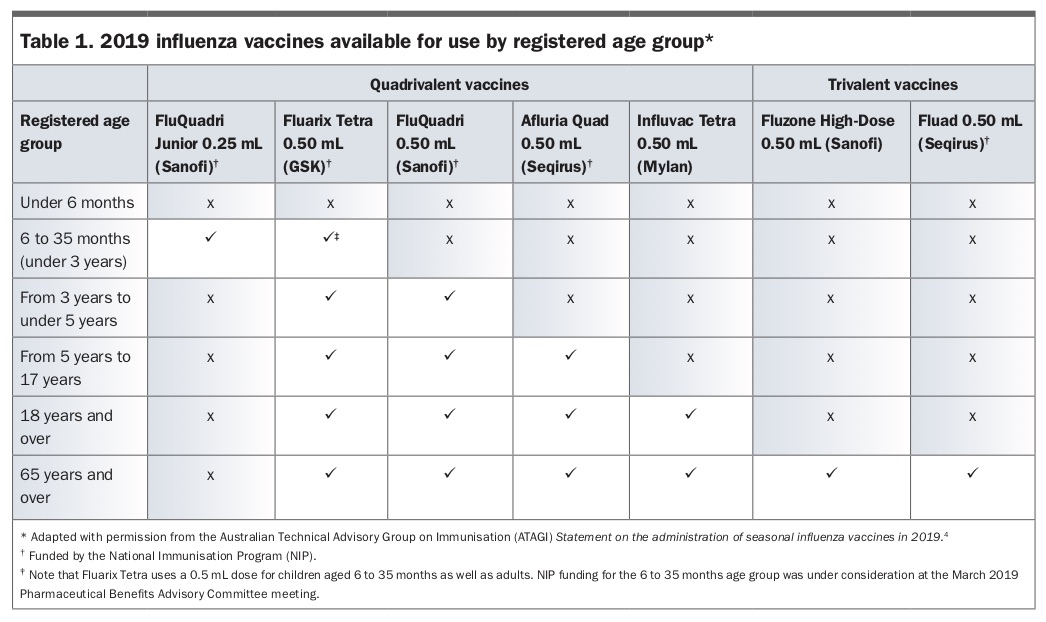
Influenza vaccines in Australia contain inactivated virus and therefore cannot cause infection. All preparations marketed in Australia in 2019 are now latex-free. Standard-dose vaccines contain 15mcg of haemagglutinin of each virus strain per 0.5 mL vaccine. Certain brands of influenza vaccines in Australia are licensed for use from 6 months of age, but others have restrictions on age. Also important is that in children aged from 6 months to under 3 years all vaccines previously used a 0.25 mL dose, but this year Fluarix Tetra uses a 0.5mL dose for all people aged from 6 months to adult. The higher antigen dose with this vaccine brand in young children under 3 years has not been associated with any significant increase in adverse events. It is important that not only the appropriate brand is used for an age group, but also that the correct dose for that brand is administered (Table 1).
{kind=link}
Enhanced influenza vaccines
To improve protection against influenza in older people during 2018, two enhanced influenza vaccines were introduced onto the National Immunisation Program (NIP) for those aged 65 years and over. Both vaccines are trivalent and do not contain a second B strain. The adjuvanted TIV (Fluad) contains MF59C.1 as an adjuvant, which boosts the immune response to the vaccine. High-dose TIV (Fluzone High-Dose) contains 60mcg of haemagglutinin (four times the standard-dose amount) for each of the three virus strains per 0.5mL of vaccine.
Both vaccines have shown around 25% greater efficacy or effectiveness than standard TIV in observational studies or randomised controlled trials conducted in influenza A(H3N2)-dominant years.18,19 As they do not include a second B strain they potentially could give less protection in a B-dominant year with the missing B strain. These vaccines are associated with slightly higher rates of local injection-site redness or soreness but similar low rates of serious adverse events compared with standard-dose vaccines. Limited data suggest small benefits over QIV.20 However, this may vary from year to year depending on the prevalence of A(H3N2) strains and any B strains covered by QIV but not by enhanced TIV. Influenza B strain-predominant seasons are less frequent than A strain-predominant ones (and more so a season with a B strain included in QIV but not TIV), and influenza B typically causes more disease in the young. Therefore, in most seasons the enhanced TIVs are likely to provide improved protection for older people compared with standard-dose QIV. Both enhanced vaccines are preferentially recommended for people aged 65 years and over in 2019, but only adjuvanted TIV will be available without charge to patients under the NIP.
Influenza vaccination recommendations
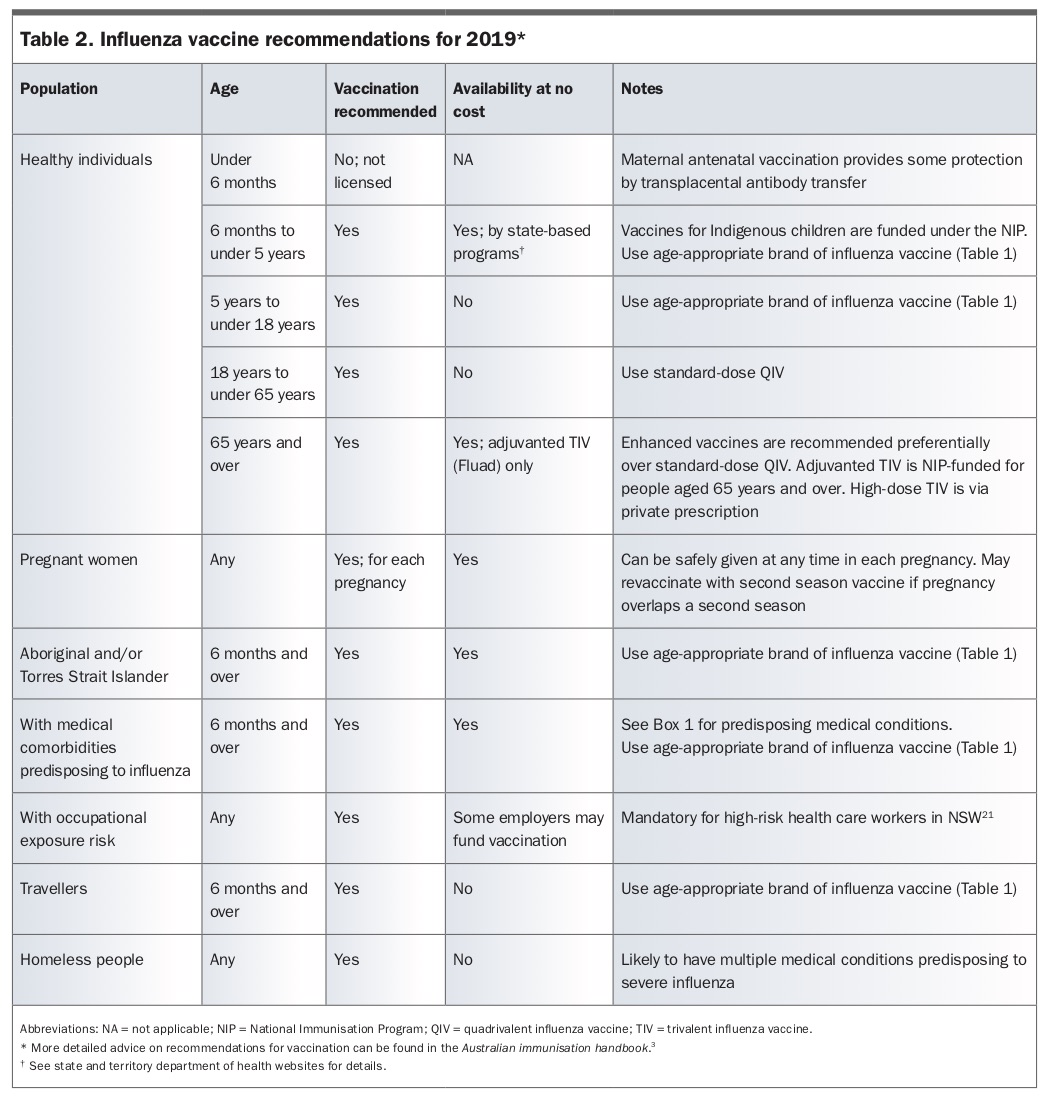
The groups recommended for vaccination in 2019 are listed in Table 2 and include all people 6 months of age and older.3,21 More detailed advice on vaccination of various groups can be found in the Australian immunisation handbook and the Australian Technical Advisory Group on Immunisation (ATAGI) Statement on the administration of seasonal influenza vaccines in 2019.3,4
{kind=link}
Of the enhanced vaccines, the recommendations do not indicate a preference for either the adjuvanted TIV or the high-dose TIV in people aged 65 years and over. Influenza vaccine is recommended for all children and has similar effectiveness in children compared with adults.22 An age-appropriate vaccine must be used (Table 1).4 Children aged under 9 years should have two doses at least four weeks apart if they have never received influenza vaccine previously. Only one dose is required if they have previously been vaccinated, regardless of whether this was in the previous season or earlier.
It is strongly recommended that health care workers (HCW), particularly those involved in aged or residential care, are also vaccinated against influenza. Vaccination of HCW prevents illness and death among patients in aged care facilities.23,24 HCW in hospitals and primary care practitioners should also consider vaccination to prevent transmission of infection to vulnerable patients. NSW Health mandates documented influenza vaccination for HCW working in high-risk clinical areas (Box 3).
{kind=link}
People who will be travelling during the influenza season domestically or internationally should receive the influenza vaccine. Those travelling in large groups, on cruises or closely confined together for days to weeks are particularly at risk. A second vaccination later in the same year to provide protection during travel in the northern hemisphere is acceptable and may be considered based on the expected risk of disease.
Vaccination is also recommended for homeless people, who often have a range of medical conditions that predispose them to severe influenza.
Funded influenza vaccination
The NIP funds free influenza vaccination for many groups including people aged 65 years and over, pregnant women, people aged 6 months and over with medical comorbidities predisposing them to influenza and all Aboriginal and Torres Strait Islander people aged 6 months and over (Table 2).3,21 In addition, in 2019, all Australian states are providing funding for vaccination of healthy children aged 6 months to under 5 years. Although the adjuvanted TIV is not recommended over the high-dose TIV, it is the only enhanced influenza vaccine that is free for people aged 65 years and over in 2019.
Timing of vaccination
Although protection from influenza vaccine is expected to last for the whole season, peak protection occurs from two weeks through to four months after vaccination, with lesser protection subsequently.25 Monitoring local patterns of influenza notifications and ensuring that adequate protection is present during the usual peak influenza season (June to September for most of Australia) ensures optimal protection. Delaying vaccination until close to the start of winter may improve protection during peak influenza season but should be balanced against the risk of missing an opportunity to vaccinate. Additionally, interseasonal influenza can occur in the spring, summer and autumn months, as occurred during early 2019 with higher than usual levels of influenza in many jurisdictions, which may signal an early start to the 2019 influenza season.1,26 It is never too late in a season for vaccination to provide appropriate protection. Pregnant women may be vaccinated at any stage of pregnancy and need not wait for a subsequent season’s vaccine; if needed, they can be vaccinated again when the new vaccine becomes available.
Safety of vaccinations
Currently available influenza vaccines have demonstrated safety in all ages for which they are TGA-approved, including during pregnancy.27 Elevated rates of febrile convulsions in young children during 2010 were shown to be associated with one brand of TIV, which was subsequently deregistered for use in children and reformulated.28 Currently, yearly active surveillance conducted by AusVaxSafety in tens of thousands of people of all ages in Australia provides assurance of vaccine safety from early each season. The results are published online weekly.29,30 In 2018, postvaccination fever rates reported by vaccine recipients or their parents were 1.5 to 1.8% in those under 5 years of age and less than 0.9% in all other age groups.30 Rates of events occurring after vaccination that had medical review were very low (less than 0.7%), and some of these were likely to have been coincidental rather than causally related to vaccination.
Contraindications to influenza vaccine are few and include previous anaphylaxis to any influenza vaccine or its components. Egg allergy (including anaphylaxis) is no longer a contraindication because reactions have been shown to be rare and mild.31 Patients with a history of previous anaphylaxis to egg can be vaccinated in a medical facility with staff experienced in recognising and treating anaphylaxis. Generally, it is recommended that patients with a history of Guillain-Barré syndrome occurring within six weeks of a previous influenza vaccination do not receive the vaccine.
Conclusion
Increased understanding of the disease burden caused by influenza across all age groups reinforces the importance of influenza vaccination at all ages from 6 months onwards. For infants too young to be vaccinated, vaccination of women during pregnancy is advantageous to both mothers and their babies. By keeping up to date with local influenza disease trends, vaccination recommendations, available vaccines and funding, immunisation providers can provide optimal care for patients and contribute to reducing the substantial burden of influenza each year. RMT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.