Reducing the burden of severe asthma

Dr Fanning is a Respiratory Advanced Trainee, Princess Alexandra Hospital, Brisbane. Professor Upham is Senior Respiratory Physician, Princess Alexandra Hospital, Brisbane; and University of Queensland, Faculty of Medicine, Brisbane, Qld.
Asthma
Breathing problems
Advanced therapies such as monoclonal antibodies improve the symptoms of severe asthma. However, the basic principles of asthma management such as optimising medication adherence, improving inhaler technique and treating comorbidities are still important.
- Severe asthma carries a high burden for affected patients and is often under-recognised.
- When standard inhaler therapies do not appear to be working, it is important to review the diagnosis and pay close attention to inhaler technique, adherence and management of comorbidities.
- New monoclonal antibodies targeting immunoglobulin E and eosinophils are now available for severe asthma and in selected patients these can markedly reduce exacerbations and oral corticosteroid use.
- In patients with a history of frequent exacerbations, high oral corticosteroid use and poor lung function, consider specialist referral.
In 2014, about one in nine people in Australia reported a diagnosis of asthma.1 The proportion of these living with severe refractory asthma is not known; however, studies from overseas found that between 3.6 and 8.1% of asthma cases were severe refractory asthma.2-4 Assuming a similar prevalence in Australia, this represents a large number of people living with severe asthma. Large gains were made in the management of asthma with the introduction of inhaled corticosteroids (ICS), but since then further reduction in disease burden has been more challenging.
The European Respiratory Society/ American Thoracic Society Task Force on severe asthma have recently updated their definition of severe asthma to: ‘asthma which requires treatment with high dose inhaled corticosteroids (ICS) plus a second controller (and/or systemic corticosteroids) to prevent it from becoming "uncontrolled" or which remains "uncontrolled" despite this therapy.’5 In Australian practice, a ‘second controller’ usually refers to a long-acting bronchodilator. Although reducing the burden of disease in those with severe asthma can be difficult, there are often gaps in treatment that can be addressed and apparent treatment resistance may have a simpler explanation. This may include an alternative diagnosis to asthma, medication nonadherence or treatment-associated comorbidities. To address this, a systematic approach (Flowchart) has been adopted to ensure all relevant issues are addressed.
Confirming the diagnosis
Asthma is defined as the presence of respiratory symptoms (e.g. dyspnoea, wheeze) due to confirmed variable airflow limitation.6 For this reason, spirometry or serial peak flow measurements are essential in the diagnosis and management of asthma, although it should be noted that normal spirometry cannot exclude asthma. However, a significant proportion of people with a diagnosis of asthma may be mislabelled.
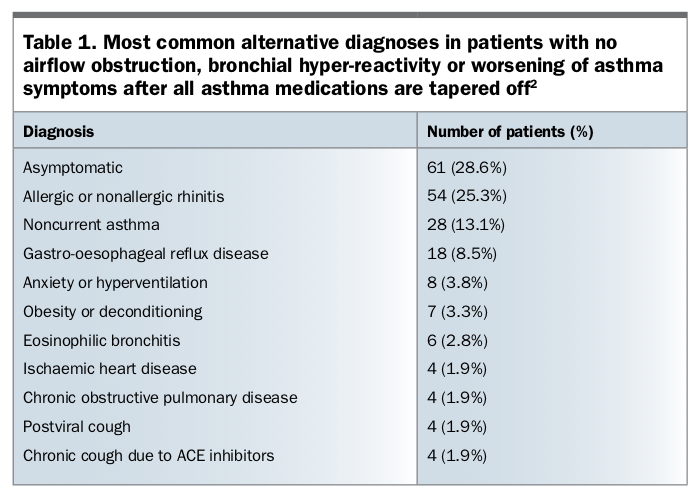
In a recent cohort study of 701 Canadian adults with doctor-diagnosed asthma, careful re-evaluation excluded current asthma in about one-third of patients.7 This may be partly explained by a high rate of spontaneous remission in asthma, but also suggests an overdiagnosis of asthma and clearly indicates that re-evaluation from time to time is needed. This is particularly prudent in those who do not appear to be responding to usual therapy. The most common alternative diagnoses in those without current asthma are listed in Table 1.2
{kind=link}
Assessing asthma control
Several validated questionnaires have been developed to assist in the assessment of asthma control including the Asthma Control Questionnaire (ACQ), Asthma Control Test (ACT) and a four-item questionnaire developed by the Global Initiative for Asthma (GINA). These are discussed in the recently developed Severe Asthma Toolkit (https://toolkit.severeasthma.org.au). These tools are easy to use in clinical practice and provide a structured way of longitudinally monitoring asthma control.
Adherence and inhaler technique
Poor adherence is a well-established contributor to poorly controlled asthma. However, it remains not only difficult to improve, but also difficult to assess objectively. Medication adherence rates among people with asthma are conservatively estimated at 50%, which is comparable to other chronic diseases such as type 2 diabetes or hypertension.8 Furthermore, adherence rates to ICS are highly dependent on the method of assessment. Patient-reported adherence is likely to be overstated when compared with more objective assessments such as dispensing records, inhaler counts or electronic adherence trackers.8
Electronic inhaler reminder devices have recently become available for a number of different inhalers. These have been shown to improve treatment adherence and reduce exacerbations in patients with asthma.9
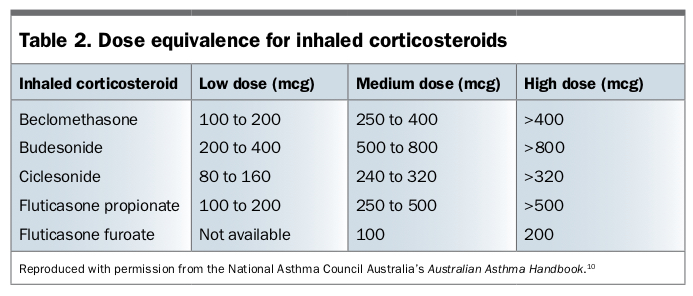
Many inhaled therapies for asthma have recently become available. Tailoring these options to the patient’s needs and preferences (e.g. frequency of dosing or preference for particular devices such as dry powder inhalers, metered-dose aerosols, spacers) may facilitate improved adherence to therapy. Importantly, the dose of ICS should be regularly reviewed and optimised based on the patient’s needs. The dose equivalence for each inhaled corticosteroid is summarised in Table 2.10
{kind=link}
Treating comorbidities
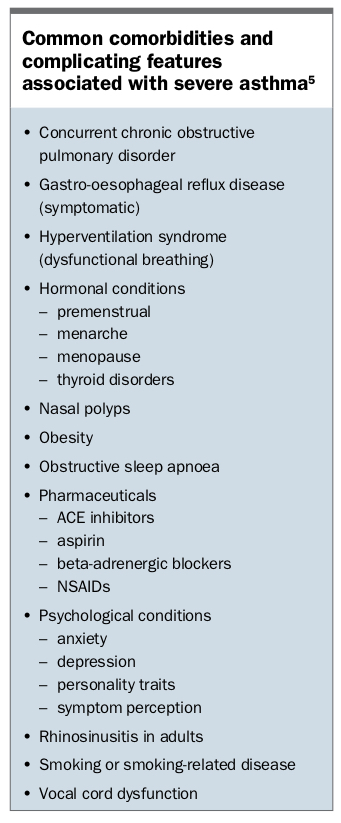
Difficult-to-treat asthma is frequently complicated by coexisting and contributory conditions (Box).5 Some of the more common and important comorbidities are discussed below. Treating these comorbidities will often obviate the need to use monoclonal antibodies.
{kind=link}
Chronic rhinosinusitis
Chronic rhinosinusitis is the most common comorbidity associated with asthma.11 It has been well established that poorly controlled sinonasal disease is associated with worse asthma control. Chronic rhinosinusitis and asthma are likely to be two manifestations of a single pathological process, based on the ‘united airways’ concept.12
The relationship between chronic rhinosinusitis and asthma may be due to several factors. First, the upper and lower airways are a continuous structure that are exposed to the same irritants, allergens and micro-organisms. Therefore, it would be reasonable to expect a similar immunological response throughout the whole respiratory tract.12 Secondly, it has been proposed that the systemic response induced by chronic rhinosinusitis, changes to the inspired air (such as reduced warming and filtering, depleted nitric oxide) caused by nasal congestion or inhalation of inflammatory mediators in sinusitis may cause an inflammatory response in the lower airway.12
Medical and surgical treatment of chronic rhinosinusitis has been shown to improve both subjective and objective measures of asthma control.13 In the case of allergic rhinitis, successful allergen immunotherapy can improve both upper respiratory and lower respiratory tract symptoms.
Smoking
A significant number of adults with asthma report that they are current smokers with rates frequently reported as similar to that of the general population. Smoking (and previous smoking) has been demonstrated in several studies to be associated with increased asthma severity and risk of asthma exacerbations.14,15 Furthermore, current smokers with asthma report more chronic cough and sputum than never or ex-smokers.16
Smoking cessation should be encouraged not only for the potential benefits in asthma but for the multitude of other health benefits. The possibility of chronic obstructive pulmonary disease as an alternative or additional diagnosis to asthma should be considered in this population.
Obesity
Obesity has complex effects on asthma, likely worsening symptoms in a multifactorial manner by increasing inflammatory mediators, altering chest wall mechanics, reducing physical activity and increasing the likelihood of comorbidities such as obstructive sleep apnoea and gastro-oesophageal reflux.
Weight loss has been associated with an improvement in asthma symptoms, and this has been replicated in multiple studies.17 This conclusion was supported in a recent systematic review, although the authors acknowledged that many studies were small so further research is needed.18
Vocal cord dysfunction and dysfunctional breathing
Vocal cord dysfunction is the unintentional adduction of the vocal cords causing respiratory distress that is not responsive to the usual treatment for asthma.19 The aetiology of vocal cord dysfunction is complex but likely involves an interplay between organic and psychological factors.19 Laryngoscopic observation of paradoxical vocal cord movement during wheezing or stridor is the gold standard procedure to confirm vocal cord dysfunction but it is often not practical.
Symptoms of vocal cord dysfunction may be very similar to asthma, but patients with vocal cord dysfunction will often localise airway narrowing to the throat and complain of more voice symptoms and fewer chest symptoms.19 Vocal cord dysfunction is often highly responsive to speech therapy and early referral of patients should be considered when suspected.19
Dysfunctional breathing refers to a chronic change in breathing pattern that results in dyspnoea in the absence of objective loss of lung function or is out of proportion with the magnitude of cardiovascular or respiratory dysfunction.20 This encompasses a broad range of dysfunctional patterns of breathing.20 Accurate identification is key to management and specialist physiotherapists and patient self-help videos have been used to improve symptoms. Breathing freely is an example of an online tool that has been shown to improve symptom control (www.breathestudy.co.uk).
Phenotyping and targeted therapies
Asthma is a broad term that encompasses many different pathophysiological types of airway inflammation (phenotypes) that produce a common syndrome. Some patients are highly allergic, some have eosinophil- dominated airway inflammation, whereas others have disease in which neutrophils seem to play an important role. Due to the development of specific therapies targeting key components of the asthma inflammatory cascade, further defining these phenotypes has become an area of interest. Of particular importance are allergic and eosinophilic phenotypes, given the currently available biological therapies.5 In selected patients, monoclonal antibodies can have dramatic clinical benefits.
Omalizumab
Omalizumab is a monoclonal antibody that targets immunoglobulin (Ig) E. IgE has been identified as a key component in the allergic asthma inflammatory cascade. By binding circulating IgE, omalizumab reduces the release of proinflammatory mediators by mast cells.21 Over the past decade, omalizumab has proven to be well tolerated and efficacious, particularly in reducing exacerbation rates and improving asthma control.21 It is most effective in patients with asthma with allergic sensitisation, and this is a prerequisite to receive a PBS subsidy for omalizumab.
One of the disadvantages of omalizumab for some patients with particularly high levels of IgE is the need for fortnightly injections. However, although omalizumab treatment is typically started in the hospital setting, it can usually be continued by the patient’s GP via subcutaneous injection. Anaphylaxis is reported but appears to be uncommon.
Monoclonal antibodies that target eosinophils
Mepolizumab and, more recently, benralizumab have become available to patients with severe eosinophilic asthma. These monoclonal antibodies are directed against interleukin (IL) 5, the main cytokine driving eosinophil differentiation. Mepolizumab targets IL-5 itself, whereas benralizumab targets the IL-5 receptor. Both agents markedly reduce the numbers of blood and airway eosinophils, and have been shown to reduce exacerbations and exposure to systemic corticosteroids.22-24
Eligibility for these agents depends on the demonstration of an elevated blood eosinophil count (≥300cells/mcL or 0.30 x 109cells/L) within the past 12 months. Both mepolizumab and benralizumab seem to be well tolerated and are often continued with the patient’s GP after injections have been initiated by a specialist. Mepolizumab is available on the PBS for uncontrolled severe eosinophilic asthma and although benralizumab has been approved by the TGA, its listing on the PBS is still under review.
Asthma control is re-evaluated after six months of all monoclonal antibody therapy with continuation dependent on clear evidence of clinical benefit (i.e. improved symptoms or reduction of long-term oral corticosteroid doses).
Specialist referral and access to further therapies
Despite optimisation of inhaled therapies and management of comorbidities, there will be a cohort of patients with treatment-resistant severe asthma. Persistently high symptom burden, two or more courses of oral corticosteroids in a year, persistently abnormal lung function or severe asthma exacerbations requiring hospital admission should trigger specialist referral of these patients. Timely referral is paramount due to the current Medicare restrictions on biological therapies, particularly the requirement for patients to be managed under a respiratory physician for at least 12 months.25
Conclusion
Asthma is a heterogeneous disease that affects a large proportion of the Australian population. Although great advancements have been made with the introduction of ICS, a systematic approach is required to continue to reduce the burden of those with resistant disease. Despite the introduction of advanced therapies such as monoclonal antibodies, this does not detract from the importance of basic principles of asthma management such as optimising medication adherence, improving inhaler technique and treating comorbidities. RMT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.