Is this uncontrolled asthma or something else?

Professor Jenkins is a Clinical Professor and Head of the Respiratory Discipline at the University of Sydney; Head of the Respiratory Group at The George Institute for Global Health, Sydney; and Senior Staff Specialist in the Department of Thoracic Medicine at Concord Hospital, Sydney, NSW.
Asthma
Breathing problems
A 43-year-old woman with a longstanding history of sinus problems, allergies and chest problems has been treated long-term for asthma. She is experiencing frequent respiratory infections that have been managed as exacerbations of asthma.
Case
Angela is a 43-year-old woman with a longstanding history of sinus problems, allergies and chest problems, principally cough and wheeze. She has a body mass index of 28.6 kg/m2. Angela was admitted to hospital at 19 years of age with asthma, and again during her first pregnancy. She has been taking fluticasone/salmeterol combination therapy 500 µg/50 µg twice daily by inhaler for many years.
Angela was under the care of an ear, nose and throat specialist and has had multiple sinus operations, the most recent being a ‘drill out’ two years ago. She reports that she had ‘grade-4 polyps and fungus in her sinuses’. Angela’s respiratory physician retired a few years ago and she has not had any ongoing specialist care for her chest problems.
Over the past 12 months, Angela has presented multiple times to various doctors at your practice with productive cough, purulent sputum, wheeze and breathlessness on exertion, with and without preceding upper respiratory tract infections. These episodes have been managed as exacerbations of asthma with inhaled short-acting ß2 agonist and oral prednisolone and, often, oral antibiotics after which her symptoms have usually improved. She has had six courses of antibiotics in the past 12 months.
A chest x-ray a few months ago was reported as essentially normal but showing some ‘mild prominence of the bronchovascular markings noted posteroinferiorly on the lateral film including some bronchial thickening’; lungs were not overinflated. A chest x-ray a few years ago was reported as showing atelectasis and mucous plugging.
Angela’s recent skin-prick test results were ‘suggestive of generalised hypersensitivity to common multiple aeroallergens’ (Alternaria spp. and Aspergillus spp. were unavailable for skin-prick testing).
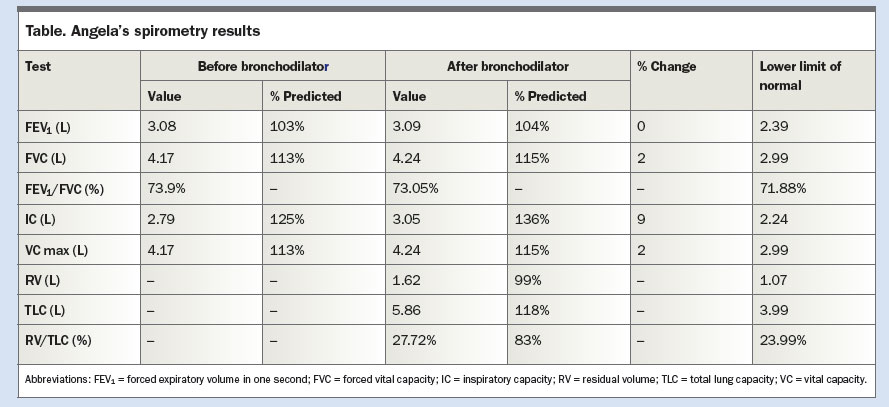
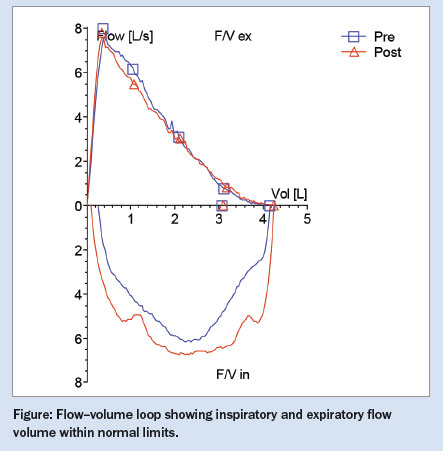
The results of recent spirometry performed at an accredited laboratory when Angela was well are shown in the Table and Figure. Angela had two puffs of salbutamol 4 hours before the test. The spirometry and flow–volume curves were normal, showing no significant acute bronchodilator response. Angela’s total lung capacity was within normal limits without air trapping, and gas transfer was normal. Her Spo2 was 94% and her modified Medical Research Council dyspnoea scale score was 1 (short of breath when hurrying on level ground or walking up a slight hill).
{kind=link}
{kind=link}
Angela is still on the waiting list to be seen by a respiratory specialist at the local public hospital. In the meantime, would it be helpful to organise any further investigations? How should these exacerbations be managed? Is this uncontrolled severe asthma, or possibly something else?
Commentary
Angela’s requirement for frequent antibiotics over the past 12 months should instantly provoke questions about her diagnosis – both whether the asthma diagnosis is correct and, if it is confirmed, whether there is something additional occurring. Although she has had two previous hospital admissions for asthma, she is on maximal therapy in the form of high-dose inhaled corticosteroid [ICS] plus long-acting ß2 agonist [LABA] therapy and is experiencing frequent lower respiratory tract infections. It would be important to know if she was taking any preventive treatment for asthma at those times, whether she has a good inhaler technique and whether she has ever had spirometry to confirm an asthma diagnosis. Additionally, lung function tests when she was well did not reveal any airflow limitation, nor did they show an acute bronchodilator response (although it would be important to know whether she had taken her fluticasone/salmeterol medication within the previous 12 hours).
Reviewing asthma medications
It is of great concern that Angela has been taking high-dose ICS plus LABA therapy for many years. This dose of fluticasone is associated with systemic effects and can rarely be clinically justified, even in severe asthma. Doses of fluticasone propionate over 250 µg a day show only very small additional benefits in reducing asthma exacerbations compared with lower doses.1 According to best practice, defined in the Australian asthma guidelines, her normal spirometry should prompt a review of this high-dose medication and a step down in dose.2
It is of concern also that she has had multiple courses of prednisone over the previous year, almost certainly for episodes that were not asthma exacerbations. She previously had completely normal lung function test results when stable, so frequent exacerbations while taking appropriate ICS plus LABA therapy would be unexpected.
Causes of recurrent infection
Recurrent respiratory infections are not normally a part of or necessarily related to having asthma, and an explanation must always be sought.
Sinus disease
One obvious possibility in Angela’s case is the seeding of infection from her sinuses, which, despite sinus surgery, may continue to be a problem because of her tendency to polyp formation. This is almost always a long-term, recurrent problem that impairs sinus drainage and predisposes a person to chronic sinusitis and, potentially, secondary infection.
Sinusitis, which commonly coexists with poorly controlled allergic rhinitis in atopic individuals, may occur independently, but also in patients with Samter’s triad, a constellation of asthma, nasal polyps and aspirin/NSAID sensitivity. These possibilities can be clarified by performing a sinus CT scan and by referral to an ear, nose and throat surgeon.
Bronchiectasis and allergic bronchopulmonary aspergillosis
Other possible explanations include the development of bronchiectasis, for which Angela’s symptoms are more typical. People with asthma are more at risk of bronchiectasis but most people with asthma do not have it. However, a syndrome of asthma with bronchiectasis, known as allergic bronchopulmonary aspergillosis (ABPA), is caused by sensitisation to Aspergillus fumigatus or, rarely, to other fungi.
ABPA is characterised by intermittent episodes of worsening asthma, often with fever, sputum plugs, haemoptysis and pleuritic pain due to mucus plugging and atelectasis. A chest x-ray may show patchy consolidation, atelectasis or collapse, and gloved-finger shadows due to mucus impacted in dilated bronchi. A high-resolution thoracic CT scan can confirm these findings and may also show central or peripheral bronchiectasis, mosaic attenuation, centrilobular nodules and tree-in-bud opacities. In acute episodes, Aspergillus precipitins is present, serum IgE is usually raised above 1000 U/mL and there may be a peripheral eosinophilia.
Angela's results
Imaging
Angela’s radiography results raise very strong suspicion of an additional issue, suggesting bronchiectasis is likely. A recent chest x-ray is reported to show ‘mild prominence of the bronchovascular markings posteroinferiorly … including some bronchial thickening’ and lungs not overinflated. A chest x-ray a few years ago was reported as showing atelectasis and mucus plugging. This earlier chest x-ray finding showed marked abnormality at a time Angela was on high-dose ICS plus LABA for asthma (assuming she was taking these as prescribed – it is essential to check adherence), strongly suggesting additional abnormalities such as ABPA or bronchiectasis, and raising the possibility that asthma is not the explanation for her symptoms.
Allergy tests
The positive skin-prick tests to several common aeroallergens are helpful in identifying atopy, however it would be important to have test results for the patient’s response to Aspergillus fumigatus, to be sure about the possibility of ABPA. A negative response to Aspergillus makes ABPA very unlikely.
Further assessment
Before finalising treatment for Angela’s bronchiectasis it is crucial to take a full history, which should include assessment of gastro-oesophageal reflux disease (GORD); elicitation of previous infections, especially childhood infections and whether she has had exposure to or active tuberculosis (TB) infection; her family history; and any history suggesting swallowing dysfunction or aspiration. Then tests should be done to assess why she may have developed this disease; in particular, quantitative immunoglobulin analysis and tests for IgG subclasses, total IgE and Aspergillus precipitins. Sputum cultures should be done to exclude TB (especially atypical TB infection) and identify treatable pathogens, especially to assess whether Pseudomonas aeruginosa is present. A thorough assessment of her sinus disease is also needed.
Finally, it is most important to determine whether Angela really has asthma and to progressively step down her asthma medication if, with hindsight, this appears no longer to be present, or, as is suggested by her lung function and symptoms, was a misdiagnosis initially. Based on her symptoms and completely normal lung function, there is no justification for the dose of ICS she is taking.
Managing bronchiectasis
Bronchiectasis should be managed by helping a patient to understand the nature of the disease and the need to undertake daily airway clearance to minimise infection risk and reduce the chance of disease progression and lung damage. Strict adherence to daily airway clearance using a huffing procedure or an oscillating positive expiratory pressure device will help reduce the risk of infections, daily cough, night-time waking and daytime sputum expectoration at unwanted times. Influenza and pneumococcal vaccination and prompt treatment with antibiotics when infections flare are very important in minimising the impact of this disease. Monthly intravenous immunoglobulin replacement is important if immunoglobulin deficiency has been identified.3 RMT
COMPETING INTERESTS: Professor Jenkins is a member of several national and international pharmaceutical company advisory boards and is paid for travel and time when attending meetings.
References
- Powell H, Gibson PG. Inhaled corticosteroid doses in asthma: an evidence-based approach. Med J Aust 2003; 178: 223-225.
- National Asthma Council Australia. Australian asthma handbook. Version 1.2. Melbourne: National Asthma Council Australia; 2016. Available online at: http://www.asthmahandbook.org.au (accessed April 2017).
- Chang AB, Bell SC, Byrnes CA, et al. Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand. A position statement of the Thoracic Society of Australia and New Zealand and the Australian Lung Foundation. Med J Aust 2010; 193: 356-365.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.