Black lung: the re-emergence of a preventable disease

Dr Ryan Hoy is a Research Fellow at the Monash Centre for Occupational and Environmental Health, Monash University; and a Respiratory and Sleep Physician at Cabrini Medical Centre and the Alfred Hospital, Melbourne, Vic.
Lung diseases
Black lung and other occupational lung diseases continue to occur in Australia. To protect workers’ respiratory health, ongoing vigilance is required to control hazardous occupational exposures.
The recent identification of black lung disease affecting coal miners in Queensland has put the spotlight on a disease that was believed to have been eradicated in Australia. Like all occupational lung diseases, black lung is preventable if adequate control measures are in place to protect workers’ respiratory health. The assumption that black lung disease had been eradicated in Australia was dispelled by the identification of eight new cases in Queensland coal miners between May 2015 and June 2016. The re-identification of black lung disease demonstrated that prevention and health surveillance systems had lapsed in this industry.
What is black lung?
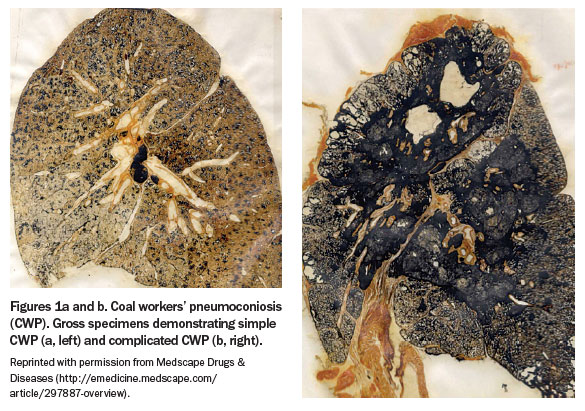
Black lung disease, formally known as coal workers’ pneumoconiosis (CWP), is so named because in severe cases the lungs literally appear black due to the high concentration of carbon deposition (Figures 1a and b).
{kind=link}
CWP is an irreversible fibrotic lung disease that is specifically caused by inhalation of coal mine dust. This dust is a mixture of carbon, silica, silicates, metals and volatile organic compounds. Cells in the lungs respond to the presence of coal dust particles by releasing proinflammatory and profibrotic mediators, stimulating pathways that lead to pulmonary fibrosis. The risk of developing CWP primarily relates to the duration and intensity of exposure to coal mine dust over a miner’s career.
Mining methods and coal dust exposure
Coal is mined from large beds or seams that are interlayered with other sedimentary rocks. If the coal bed is located more than 60 metres underground, it is generally accessed by an underground method rather than through open cut mining. The enclosed underground environment significantly increases the risk of coal mine dust accumulation.
In Queensland, most underground mines use the longwall mining method, where a machine cuts across the coalface causing coal to fall onto a conveyor belt for transport. A hydraulic system supports the roof, which advances with the cutting. This process allows large beds of coal to be totally extracted and generally is more productive than other methods. However, longwall mining can produce four times as much coal mine dust as other methods, particularly when production rates are high.1
Occupational safety measures
In developed countries, the incidence of CWP decreased markedly during the 20th century due to increased automation of mining, introduction of dust exposure limits, use of personal protective equipment and improvements in dust management. Unfortunately, in developing countries these advances have not yet fully occurred and CWP is still a major health problem. A recent report from Colombia, which is now a major international exporter of coal, found a CWP prevalence of 36% among miners.2
Diagnosis and course of disease
The diagnosis of CWP can be challenging. Workers with early stage disease (simple CWP) are usually asymptomatic and may be detected incidentally or through workplace health surveillance. Radiologically, simple CWP is characterised by small nodules most commonly involving the upper and mid-zones of the lungs.
Simple CWP progresses to complicated CWP when nodules become greater than 10 mm in size (Figure 2). Nodules may merge to form conglomerated masses with associated loss of lung volume. This severe form of disease is known as progressive massive fibrosis. Respiratory function tests may show obstructive, restrictive or mixed ventilatory defects depending on the severity and pattern of disease.
{kind=link}
Symptoms
Symptoms associated with CWP usually begin insidiously many years after initial exposure to coal mine dust, not uncommonly after the miner has left the industry. This long latency can result in failure to recognise the association of the past exposure with the current disease.
Respiratory symptoms of CWP are nonspecific. If disease advances, symptoms progress from mild cough, followed by increasing breathlessness, wheeze and cough productive of black sputum (melanoptysis). Late stage CWP is associated with an increased risk of pulmonary hypertension, cor pulmonale and death.3 The cumulative amount of coal mine dust exposure experienced by a worker is the primary factor associated with the risk of disease progression.
Respiratory comorbidities
Apart from CWP, exposure to coal mine dust can also cause emphysema, chronic bronchitis and diffuse dust-related fibrosis. ‘Coal mine dust lung disease’ is the preferred umbrella term that encompasses this range of diseases.
A history of tobacco smoking is not uncommon among current and former coal miners; however, this history does not rule out the presence of an occupational cause of lung disease and should not deter further evaluation. When a history of multiple hazardous exposures is present, it can be very challenging to determine the proportion of disease and disability caused by the separate exposures.
System failures in Queensland
Following the identification of CWP cases in 2015 and 2016, Monash University was commissioned by the Queensland Government to undertake a review of the Queensland Coal Mine Workers’ Health Scheme. The review identified major system failures in the design and operation of the scheme.1
Health surveillance is recommended when workers undertake activities that may involve exposure to respiratory hazards. The aim of health surveillance is to detect early markers that provide an opportunity for intervention that may prevent disease establishment or progression. In the setting of exposure to coal dust, surveillance involves periodic medical examinations, respiratory function tests and chest x-rays. Abnormal findings suggest that there may be failings of control measures at the workplace and should trigger review of the adequacy of those measures. Health surveillance is particularly important in a condition such as CWP, where at the early stages of disease workers will be asymptomatic and intervention may lessen the chance of disease progression.
The Monash review noted inadequate training of doctors performing health assessments and found that chest x-rays and spirometry were frequently of poor quality and/or were interpreted inadequately.1 The scheme lacked systems to ensure workers were monitored over the course of their careers and clear protocols to direct evaluation of workers with abnormal results.
Preventing occupational disease
The proportion of lung disease that is caused by occupational exposures is underappreciated. Current estimates have indicated that 10 to 15% of COPD, 15% of adult-onset asthma and 5 to 10% of lung cancers are attributable to occupational exposures.4-6
Managing respiratory hazards requires a comprehensive approach. Health surveillance is one aspect of this, but the most important is controlling the generation of the hazard at the source. In the coal mining industry, this involves ensuring that dust control strategies are optimal and that dust levels are frequently monitored in the work environment to ensure that the control measures are effective. In coal mines, these measures include dust suppression water sprays, ventilation systems and airborne dust collectors, such as scrubbers. Face masks should never be relied on as an effective protective measure because masks are prone to poor fitting and are difficult to wear, especially when performing physically demanding tasks such as mining.
Conclusion
Fortunately, many lessons are being learnt from the identification of CWP among Queensland coal miners. One of the most important of these is that CWP is a disease that is not just of historical interest. Old and new occupational lung diseases continue to occur in Australia, silicosis and asbestos-related cancer being other examples. Ongoing vigilance is required to identify occupational causes of lung disease and to ensure optimal workplace health and safety practices are in place to protect workers’ respiratory health. RMT
COMPETING INTERESTS: None.
References
- Monash Centre for Occupational and Environmental Health and University of Illinois School of Public Health. Review of the respiratory component of the Coal Mine Workers’ Health Scheme for the Queensland Department of Natural Resources and Mines. Final report: Melbourne; Monash University; 2016.
- Torres Rey CH, Ibanez Pinilla M, Briceno Ayala L, et al. Underground coal mining: relationship between coal dust levels and pneumoconiosis, in two regions of Colombia, 2014. BioMed Res Int 2015; 2015: 647878.
- Zosky GR, Hoy RF, Silverstone EJ, et al. Coal workers’ pneumoconiosis: an Australian perspective. Med J Aust 2016; 204: 414-418.
- Fishwick D, Sen D, Barber C, et al. Occupational chronic obstructive pulmonary disease: a standard of care. Occup Med (Lond) 2015; 65: 270-282.
- Toren K, Blanc PD. Asthma caused by occupational exposures is common – a systematic analysis of estimates of the population-attributable fraction. BMC Pulm Med 2009; 9: 7.
- Consonni D, De Matteis S, Lubin JH, et al. Lung cancer and occupation in a population-based case-control study. Am J Epidemiol 2010; 171: 323-333.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.