Occupational lung diseases: why an occupational history is important

Dr Barnes is a Respiratory and Sleep Physician at the Alfred Hospital, Melbourne; and a Research Fellow at the Central Clinical School and Monash Centre for Occupational and Environmental Health, Monash University, Melbourne. Dr Hoy is a Respiratory and Sleep Physician at the Alfred Hospital Occupational Respiratory Clinic, Melbourne; and a Senior Research Fellow at the Monash Centre for Occupational and Environmental Health, Monash University, Melbourne, Vic.
Lung diseases
Occupational respiratory exposures contribute significantly to the burden of lung disease in Australia. Although an occupational history should be obtained from all patients presenting with respiratory symptoms, it is often overlooked. Identification of contributory occupational exposures can improve outcomes for individual patients and may also have important public health implications through identifying unsafe work practices.
- An occupational history is often missed in people presenting with respiratory symptoms.
- Respiratory diseases such as asthma, chronic obstructive pulmonary disease and interstitial lung diseases, including silicosis and hypersensitivity pneumonitis, have strong associations with occupational exposures.
- Respiratory symptoms that are worse at work and improve when away from work are highly suggestive of a workplace-related respiratory disease.
- Confirming the association between an occupational exposure and a disease, and subsequently controlling exposure, are important components of management and may help cure or prevent further exacerbation of disease, as well as protect other workers.
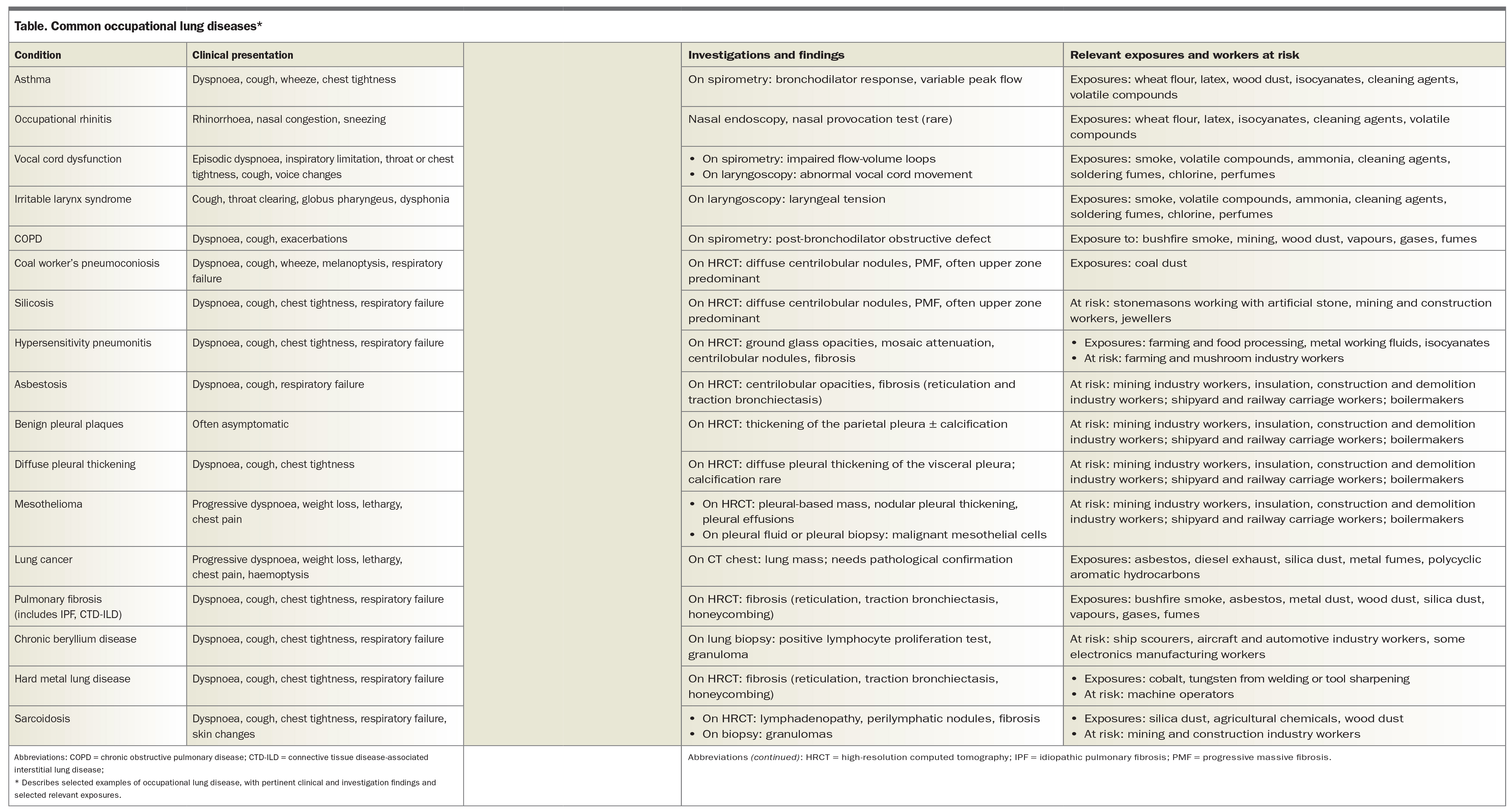
Occupational lung diseases comprise many respiratory conditions that are caused or exacerbated by inhalational exposures in the workplace. Respiratory diseases secondary to workplace exposures are common; internationally, 15% of adult-onset asthma, 15% of chronic obstructive pulmonary disease (COPD) and 10 to 30% of lung cancer cases are attributable to workplace exposures.1-5 The contribution of workplace exposures to respiratory disease is underappreciated because they are not always assessed. Making the link between exposure and illness can improve patient outcomes and may even prevent chronic illness, yet the occupational history is often overlooked. A UK study found that only one in seven GPs recorded an occupation for their patients with asthma.6 When evaluating any respiratory symptom or disease, clinicians need to consider occupational exposures as potential contributing factors. This review highlights common occupational lung diseases in Australia and outlines the most important points in taking an occupational history. A summary of common occupational lung diseases and their presentations, treatment and relevant exposures is presented in the Table.
{kind=link}
Work-related asthma
Work-related asthma is one of the most commonly encountered workplace-related respiratory diseases and is potentially preventable. Work-related asthma includes:
- occupational asthma, which is new-onset asthma, or the recurrence of previously quiescent asthma, specifically caused by workplace conditions
- work-exacerbated asthma, defined as the worsening of the control of pre-existing asthma due to workplace factors.7
Dyspnoea, chest tightness, wheeze, cough and increased use of reliever medication when at work and improvement in symptoms when not at work (such as weekends or holidays) are highly suggestive of work-related asthma.8-10
Work-related asthma may be due to allergic or, less commonly, nonallergic exposures. Allergic asthma is caused by exposures to specific allergens, known as asthmagens, which sensitise the airways. A multitude of occupational asthmagens have been reported, the most common of which in Australia include wheat flour, natural rubber latex, agricultural exposures and cleaning agents.11 Nonallergic or irritant-induced asthma is less common, and is caused by moderate to high levels of exposure to respiratory irritants including fumes, gases and volatile compounds.12
The initial step in the investigation of possible work-related asthma is to confirm that asthma is the cause of the presenting respiratory symptoms. Pre- and post-bronchodilator spirometry may confirm variable airflow obstruction; however, for some patients, a bronchial provocation challenge, such as with methacholine or mannitol, is needed.7 A detailed discussion on the diagnosis of asthma is provided by the Australian Asthma Handbook (www.asthmahandbook.org.au/). To establish a relationship between the onset of asthma symptoms and the work environment, peak flow measurements that show variability at work and away from work are useful. The diagnosis of work-related asthma can be challenging, and referral to a respiratory physician with expertise in occupational lung disease should be considered.
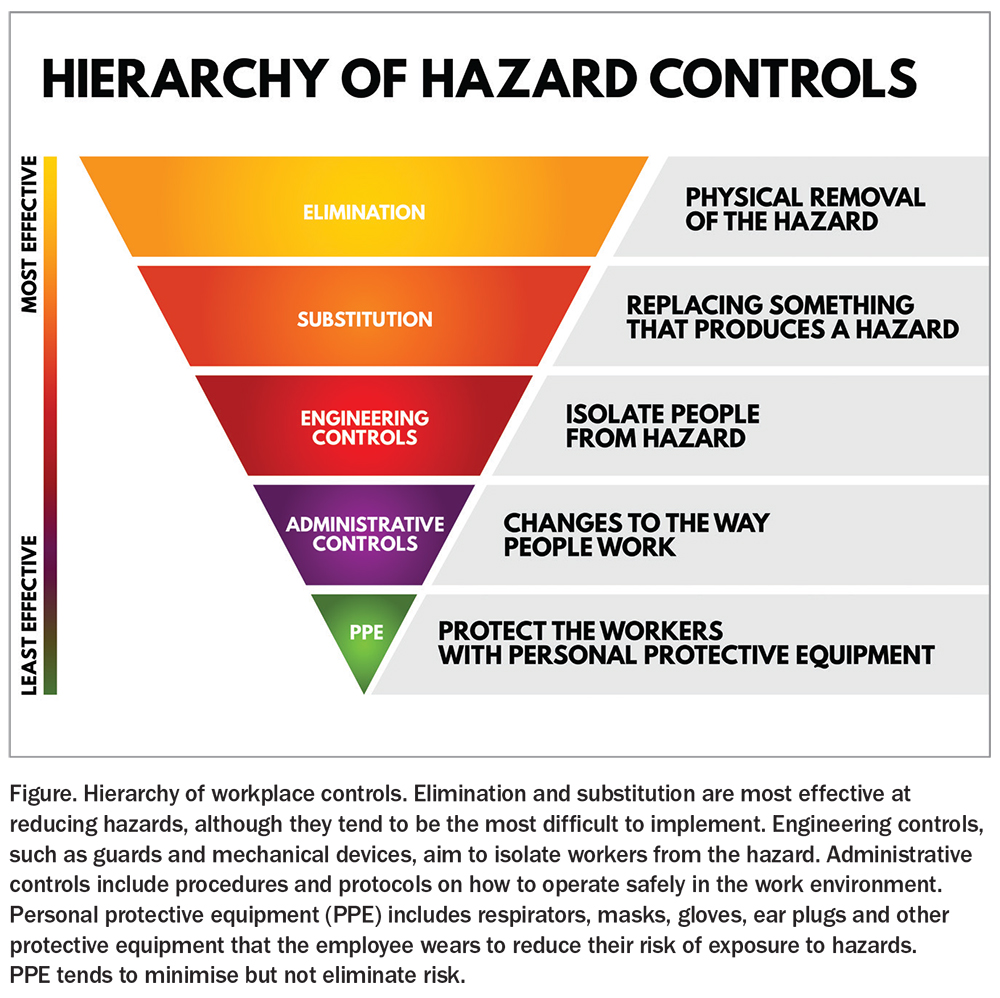
Complete avoidance of the causative exposure may cure or substantially improve asthma symptoms. Avoiding exposure may require the patient to change their role, job or workplace; however, the social and financial implications of this decision need to be considered before making this recommendation. Preferably, the employer should thoroughly investigate and completely control the causative workplace exposure (e.g. switching to latex-free gloves), which will also reduce the risk to other workers (Figure). Patients who continue to work in an environment with potential ongoing exposure are at risk of significant decline in lung function and worsening asthma control and therefore require regular medical review.7 More information on occupational asthma is available on the Severe Asthma Toolkit website (https://toolkit.severeasthma.org.au/diagnosis-assessment/triggers-occupational-asthma/).
{kind=link}
An important mimic of work-related asthma is irritable larynx syndrome, which can cause a range of symptoms including chronic cough and episodic shortness of breath triggered by irritants, fumes and strong odours.13 Vocal cord dysfunction (also known as inducible laryngeal obstruction), which is a component of irritable larynx syndrome, is characterised by inappropriate, transient and reversible narrowing of the larynx in response to external triggers.14 Patients describe episodic dyspnoea, particularly with inspiration, throat tightness and cough.13 Specialist assessment is often needed to differentiate between work-related asthma and irritable larynx syndrome.
Chronic obstructive pulmonary disease
Although mostly associated with smoking, work exposures contribute substantial risk in the development of COPD. It is estimated that 10 to 20% of COPD cases, both in Australia and worldwide, are associated with occupational exposure.3,15 Dust and fume exposures (e.g. from mining, wood dust, vapours, gases, fumes, bushfire smoke) are often implicated.4,15,16
When assessing a patient with COPD, clinicians need to ask about previous occupations as well as current roles, as COPD can present many years, if not decades, after the causative exposure. It may be difficult to distinguish the contribution of occupational exposures from other environmental exposures such as smoking. Lung function tests showing an obstructive defect post-bronchodilator confirm the diagnosis of COPD.17 Treatment includes pharmacological and nonpharmacological therapies, in addition to avoiding contributing factors such as workplace exposures and smoking.17
Occupational interstitial lung diseases
Occupational interstitial lung diseases (ILDs) occur when inhaled dust particles become lodged in the lungs, resulting in scarring. Occupational-related ILDs include pneumoconioses (silicosis, coal worker’s pneumoconiosis), hypersensitivity pneumonitis and granulomatous lung diseases.
Pneumoconioses
Pneumoconioses are diffuse ILDs caused by dust exposure. Although workplace control measures have reduced the incidence of many of these diseases over time, there has been a recent resurgence of coal worker’s pneumoconiosis and silicosis in Australia. Coal worker’s pneumoconiosis causes cough, dyspnoea, melanoptysis (black-pigmented sputum), pulmonary function defects (obstructive, restrictive or mixed) and interstitial changes on CT chest imaging.18,19 An increase in pneumoconiosis cases was reported in Queensland in 2016 due to inadequate mining workplace controls, failures of health surveillance and lack of adherence to regulatory standards.19
Silicosis
Silicosis is caused by the inhalation of silica dust. The incidence of silicosis has recently increased sharply in Australia.20 This is largely because of the use of engineered or artificial stone to produce fashionable kitchen benchtops. Engineered stone has an extremely high silica content of over 90%. When this stone is cut, shaped and polished by workers, high levels of respirable crystalline silica dust are generated. Traditionally, silicosis required decades of exposure before disease developed; however, workers are now developing silicosis after only a few years (two to 10 years) in this industry.21,22
Because of this outbreak, many states and territories in Australia have implemented active screening programs for those working in the stone benchtop industry. Patients with silicosis often have no symptoms at the time of diagnosis; however, they may report chest tightness, cough and progressive dyspnoea. CT chest features include ground glass centrilobular nodules in the early stages. Over time, these nodules can coalesce to form progressive massive fibrosis.23 A good clinical history is essential in these patients, as appearance on CT may be similar to sarcoidosis and other connective tissue disease-related ILDs.
Workers’ compensation is usually available for those working in the stone benchtop industry who develop silicosis, and these patients should be encouraged to change to a different industry, as ongoing silica exposure is linked to disease progression.24,25 Some patients may, however, have progressive disease even after cessation of exposure.26 At present, limited treatment options are available for patients with silicosis; some require lung transplantation, therefore, prevention and exposure reduction are essential to reduce disease progression.
Hypersensitivity pneumonitis
Hypersensitivity pneumonitis (HP) is an immune-mediated ILD caused by inhalational exposures. Certain low-molecularweight organic compounds commonly cause HP. The most common workplace-related exposures include farming, wood dust, mould (e.g., from hot tubs, water damage in buildings) and food processing (e.g. mushroom and farming industries). Inorganic low-molecular-weight chemicals, such as isocyanates, although themselves not immunogenic, can combine with human proteins to form haptens and trigger HP.27,28 Other exposures that may cause HP can be found on the HPLung website (www.HPLung.com). Patients may present with acute-onset fevers, dyspnoea, cough and malaise. In the later stages, progressive dyspnoea and respiratory failure can develop, with ground glass opacity, mosaic attenuation and fibrosis seen on CT imaging.29
Asbestos-related lung diseases
Asbestos-related lung diseases include asbestosis, a type of ILD with a similar CT pattern to idiopathic pulmonary fibrosis; pleural disease, ranging from benign pleural plaques to diffuse pleural thickening with associated reduction in lung volumes, dyspnoea and chest wall pain; mesothelioma, a progressive malignant disease with a poor prognosis; and lung cancer.
Australia has a disproportionately high incidence of asbestos-related lung disease, which is a reflection of the extent of asbestos use in the mining and manufacturing industries up until complete cessation of use in 2003.30 Those who worked in mining, insulation, boilermaking and cement production industries, as well as shipyard workers and railway carriage workers, are at greatest risk of developing asbestos-related lung diseases. Those who currently perform demolition and asbestos removal without adequate protection are also at risk.30 Asbestos-related lung disease is often compensable, and consultation with the state- or territory-specific workplace health and safety regulator or a workers’ compensation lawyer can provide guidance on how to seek compensation.
Other ILDs
Rarer ILDs that result from specific occupational exposures include chronic beryllium disease and hard metal disease (Table).31,32 Occupational exposures also contribute substantially to the development of other ILDs, including idiopathic pulmonary fibrosis, connective tissue disease-related ILDs and sarcoidosis.33-35
{kind=link}
Taking an occupational history
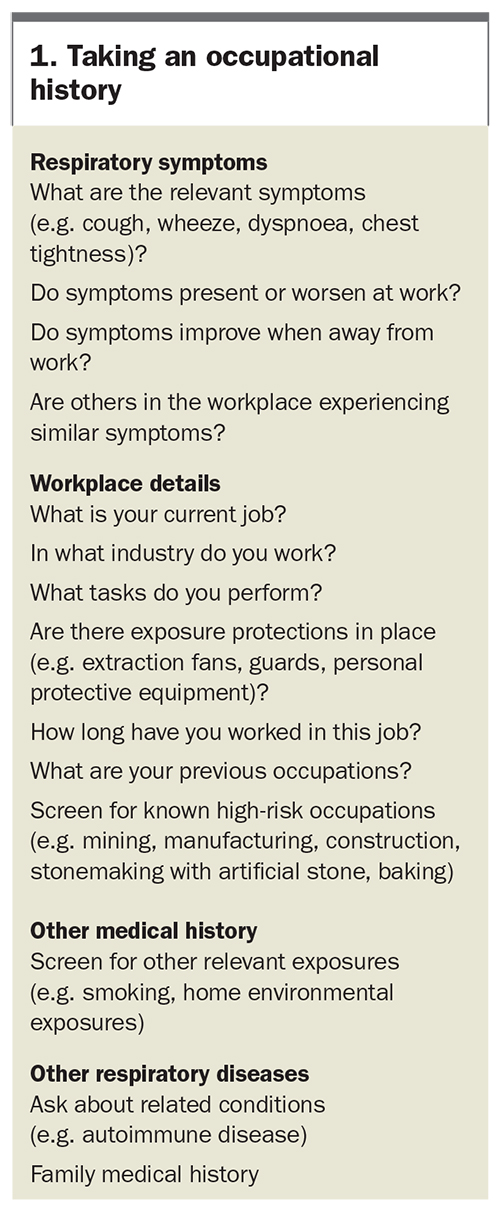
All clinicians need to have knowledge about what their patients do or have done for work. When taking a more detailed occupational history, clinicians should ask about the patient’s current job, what tasks are involved and in what industry they work (Box 1). Respiratory symptoms that worsen at work and improve when away from work are highly suggestive of some occupational lung diseases, in particular, allergic diseases. Clinicians should also ask if other people in the workplace have been affected by similar symptoms or diagnosed with lung disease. Clinicians should also consider if the patient works in an occupation with known high occupational risk (e.g. working in mining, or as a stone mason or baker), and what protective measures are in place. Previous occupations should also be recorded, especially when a condition with long latency (e.g. COPD, asbestosis) has been identified. In addition to an occupational history, clinicians should ask about potentially relevant home and hobby exposures (e.g. mould in the home, or bird keeping or woodwork as a hobby) and other potentially relevant respiratory exposures (e.g. smoking, vaping).
{kind=link}
Further investigations
Further investigations will be directed by the presenting symptoms and the diagnoses that are being considered. Further studies may include lung function tests and CT imaging. Lung function tests may reveal an obstructive (asthma, COPD), restrictive (asbestosis, HP, IPF) or mixed (pneumoconiosis) pattern. A significant bronchodilator response may indicate work-related asthma. In those with suspected work-related asthma, peak flow monitoring should be performed daily, at and away from work, to show airflow variability. High-resolution CT chest imaging may reveal parenchymal lung disease in patients with asbestosis, pneumoconiosis and other ILDs.
How should occupational lung disease be managed?
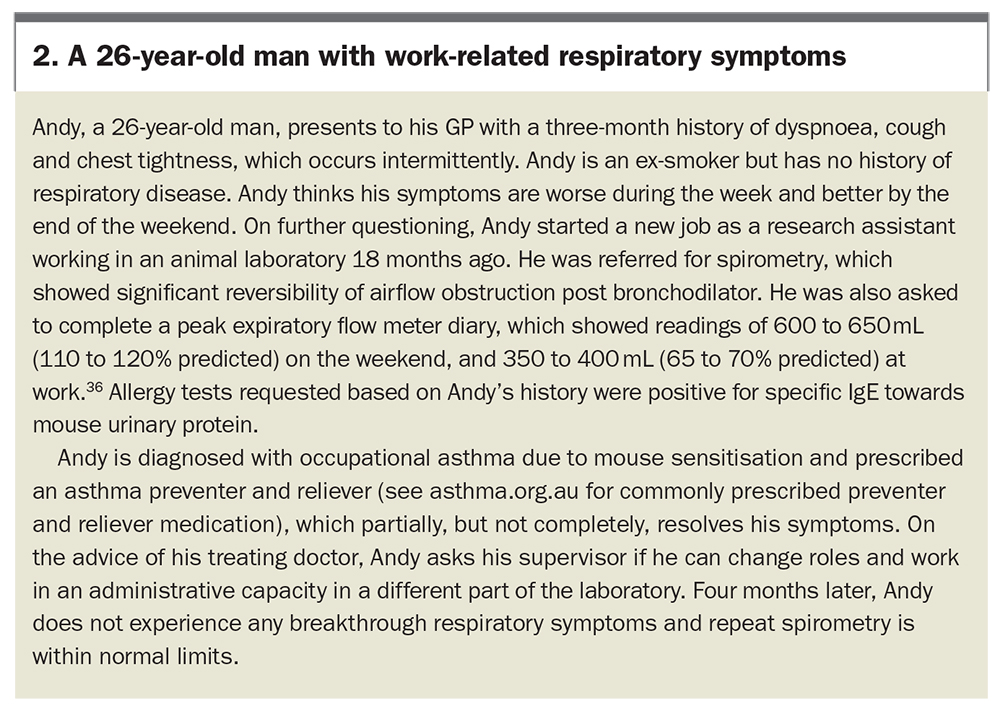
Referral to a respiratory physician with expertise in occupational lung disease or, if available, an occupational lung disease clinic, may be needed to confirm a diagnosis and guide management. Management of occupational lung diseases requires clear communication with the patient and employer. If the current job is causing symptoms, patients may be advised to seek other roles in the same industry or change industries altogether. A case vignette of a patient with work-related respiratory symptoms is presented in Box 2.36
{kind=link}
Typically, workers’ compensation insurance is available after the diagnosis of an occupational lung disease and may assist with retraining and identification of suitable alternative work. The diagnosis of an occupational lung disease can be highly stressful for patients and they will often need counselling and psychological support. Personal protective equipment, such as a respirator, is the least effective workplace control measure and should never be recommended as the only intervention for a patient with occupational lung disease (Figure). Other general aspects of the management of occupational lung diseases are similar to lung diseases that are not work related, and include smoking cessation, vaccinations and exercise programs.
Conclusion
Hazardous occupational exposures contribute substantially to the burden of respiratory disease in Australia. Taking an occupational history is often overlooked, but needs to be performed in any patient presenting with respiratory symptoms or disease. Identifying hazardous occupational exposures has important implications for the patient’s health, as well as potentially reducing future risk to other workers. Patients may consider avoiding current exposures as part of their management plan. Referral to specialists with respiratory and occupational expertise can assist in the diagnosis and ongoing management of these patients. RMT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.