Pulmonary nodules: evaluation in general practice

Dr Leong is a Respiratory and Sleep Physician at Austin Health, Melbourne; and Clinical Senior Lecturer at the University of Melbourne, Melbourne, Vic. Professor Brims is a Respiratory Physician at Sir Charles Gairdner Hospital, Perth; Professor at Curtin University, Perth; and Deputy Director of the Institute for Respiratory Health, Perth, WA.
Lung cancer
Lung diseases
Pulmonary nodules are increasingly detected as incidental findings or through lung cancer screening programs. GPs play a key role in the appropriate evaluation of nodules, specifically in identifying those with a high probability of cancer that require timely multidisciplinary referral.
- The incidence of pulmonary nodules is increasing.
- Five percent of pulmonary nodules represent early-stage lung cancer, which is potentially curable.
- The probability of a nodule being malignant can be calculated from patient and nodule characteristics.
- Guidelines provide recommendations for follow up based on the probability of malignancy.
- Timely referral to a specialist for discussion at a lung cancer multidisciplinary team meeting is important if a nodule has an intermediate to high risk of malignancy, or if the GP has concerns.
- Care must be taken to alleviate patient anxiety during nodule evaluation.
- Smoking cessation is strongly recommended in all smokers undergoing nodule evaluation.
Pulmonary nodules are defined as focal radiological opacities of the lungs that measure less than 30 mm in diameter. Increasing sensitivity and frequency of chest imaging modalities such as CT have resulted in greater incidental detection of pulmonary nodules.1 Additionally, the implementation of lung cancer screening programs has led to higher numbers of screening-detected nodules.2,3
Although about 95% of nodules are benign, an important minority represent lung cancer. Lung cancer continues to be the leading cause of cancer death in Australia, largely because patients are often diagnosed at an advanced stage, when cancer has metastasised to regional lymph nodes and distant organs.4 Therefore, appropriate evaluation and management of nodules can result in detection of cancer at an early stage when it may still be potentially curable. Here, we describe approaches to pulmonary nodules discovered incidentally or detected through screening and the important role of GPs in the assessment pathway.
Approach to pulmonary nodules discovered incidentally
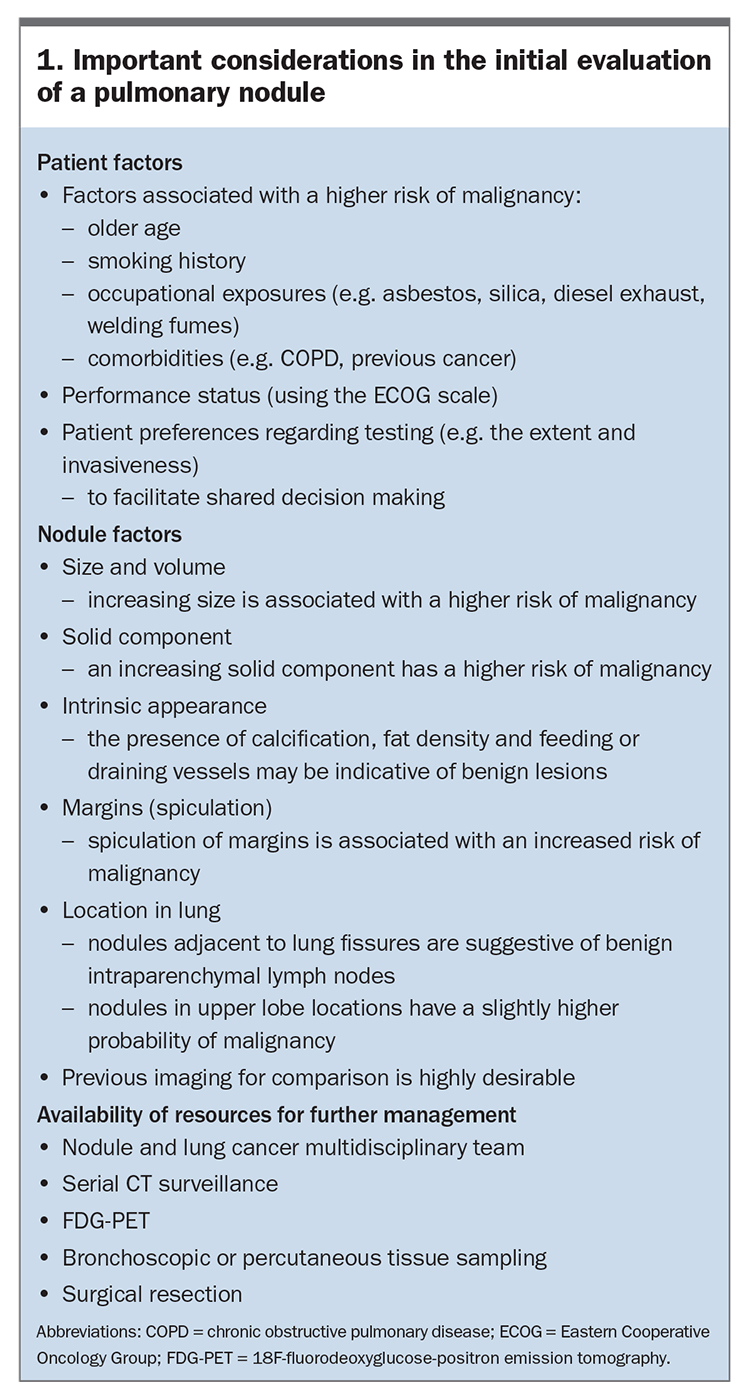
Incidental pulmonary nodules are commonly detected on imaging that has been performed for unrelated indications. For example, in a review of 1000 CT pulmonary angiograms requested for suspected pulmonary emboli, incidental nodules were observed in 10% of studies.5 Occasionally, a nodule may be detected incidentally without adequate (full) imaging of the lung fields and upper abdomen, in which case a formal CT chest may be required to ensure proper radiological assessment. The clinical assessment of an incidental nodule should involve a personalised assessment (Box 1), including the nature and risk profile of the nodule itself, background lung cancer risk of the patient (age, smoking status, family history, occupational exposures), comorbidities and patient preference, as well as an understanding of the local availability and diagnostic yield of further tests (Flowchart).6,7,8
{kind=link}
Patient factors
Patient factors associated with higher frequency of malignant pulmonary nodules include: increasing age; smoking history; occupational exposure to carcinogenic agents; and comorbidities, such as chronic obstructive pulmonary disease (COPD) and prior extrathoracic malignancy.9,10 Presenting symptoms that constitute red flags include unexplained or nonresolving cough, haemoptysis, unintentional weight loss and slow-to-resolve chest infections. However, it is important to acknowledge that most pulmonary nodules are asymptomatic.
Nodule characteristics
Certain nodule characteristics are associated with malignancy. The probability of malignancy is lower than 1% in nodules measuring less than 6 mm; however, it rises to 1 to 2% in lesions that are 6 to 8 mm, and almost 10% in nodules over 8 mm.9-11 Nodules are categorised according to their appearance as solid, part-solid or nonsolid (often described as having a ‘ground-glass’ radiological appearance). A part-solid nodule with an increasing solid component over time has a higher risk of malignancy, likely representing adenocarcinoma in situ.9 Intrinsic features of calcification, fat and feeding or draining vessels may be indicative of benign lesions, such as granuloma, hamartoma and arteriovenous malformation, respectively.9 Spiculation of the margin is independently associated with an increased likelihood of cancer.10 Lastly, nodules adjacent to lung fissures are suggestive of benign intraparenchymal lymph nodes, compared with nodules in upper lobe locations, which have a higher probability of malignancy.12
Accessing previous CT imaging is crucial in the assessment of an indeterminate nodule. Stability in nodule size and characteristics (for more than two years for a solid nodule and for more than five years for a nonsolid or part-solid nodule) indicates the nodule is likely benign. Volume doubling time can be calculated using previous imaging, with less than 400 days considered a fast-growing nodule likely to require further investigation.13 If no previous imaging is available, the present CT date should be considered the ‘index CT’ and follow-up commenced from that date for the periods above (solid: two years; nonsolid and part-solid: five years).14,15 Positron emission tomography (PET)-CT is frequently unhelpful with small and part-solid or nonsolid nodules, and a ‘negative’ PET scan should not be a reassurance to clinical teams or patients.16
Further investigation and management of nodules
Various professional societies have developed guidelines with recommendations on how to manage pulmonary nodules based on the estimated risk of malignancy. Of these, the Fleischner Society guidelines for managing incidental pulmonary nodules are the most frequently used in Australia (https://pubs.rsna.org/doi/full/10.1148/radiol.2017161659).14 Nodules are categorised as being low- or high-risk of malignancy according to nodule size (calculated as the mean of long and short diameters: 6 mm, 6 to 8 mm, greater than 8 mm), number (single vs multiple) and appearance (solid vs part-solid).
Based on these features, recommendations include: nodule surveillance with serial CT imaging; metabolic imaging with 18F-fluorodeoxyglucose-positron emission tomography (FDG-PET); minimally invasive tissue sampling via bronchoscopic or transthoracic approaches; and surgical resection, which is simultaneously diagnostic and therapeutic.14,17,18
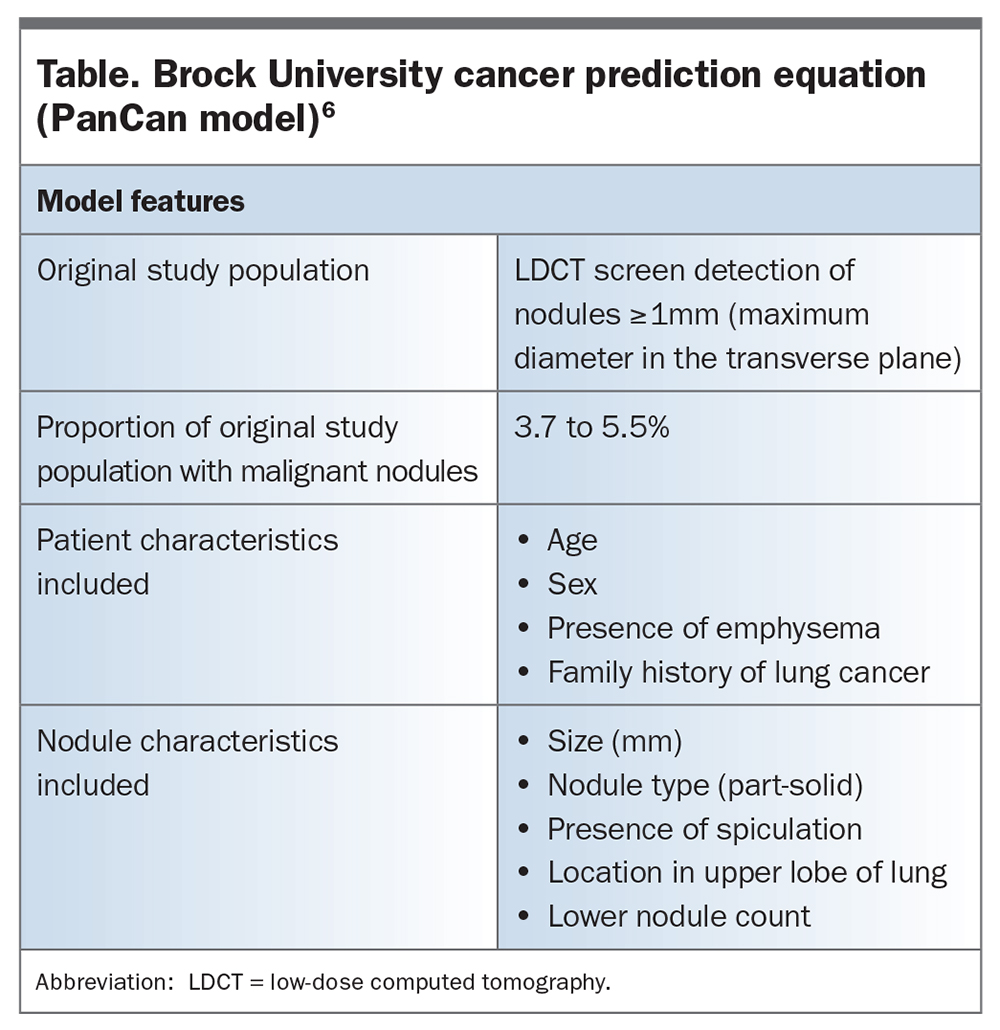
Furthermore, several mathematical risk calculators have been developed to help distinguish malignant nodules from benign nodules. In Australia, the Brock University cancer prediction equation, also known as the PanCan model, is widely used and is the most likely to be adopted if a lung cancer screening program is implemented in Australia (Table).6,19-21 It is available at: https://www.uptodate.com/contents/calculator-solitary-pulmonary-nodule-malignancy-risk-in-adults-brock-university-cancer-prediction-equation. A threshold of a 10% malignancy risk guides the management of each nodule. CT surveillance is generally appropriate if the nodule has a low probability (less than 10%) of malignancy, if other testing is considered high-risk or low diagnostic yield, or if a patient prefers a more conservative approach.9 In cases of intermediate probability (10 to 70%) of malignancy, FDG-PET may provide metabolic information and radiological staging.9 However, false negatives may occur in nodules that are less than 10 mm or slow-growing, and false positives may arise in the setting of infection or inflammation. Tissue sampling may also be considered in cases of intermediate risk of malignancy, when the sampling modality depends on the location of the nodule, patient fitness for the procedure and the local resource availability.9 Advances in bronchoscopic technology have enhanced the ability to navigate to small peripheral pulmonary nodules, with less risk of pneumothorax compared with transthoracic biopsy.22 When the risk of malignancy is high (greater than 70%), and/or with a growing nodule on two consecutive CT scans, proceeding to surgical resection without prior tissue diagnosis may be considered.9 For patients deemed medically unfit for surgery, or patients preferring noninvasive management, stereotactic ablative body radiotherapy is a highly effective approach that involves delivery of a high irradiation dose to a precise target area.18
{kind=link}
Indications for specialist referral
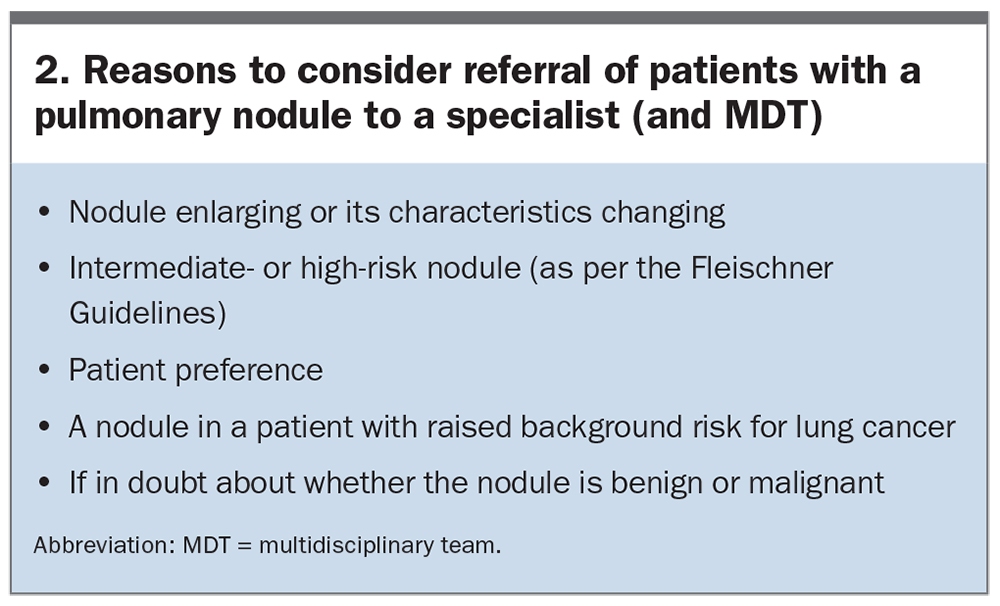
Nodule characteristics that should constitute red flags for specialist referral are described in Box 1 and include increasing size, increasing solid component and spiculation of the margin. Referral to a specialist who is affiliated with a lung cancer multidisciplinary team (MDT) should always be undertaken if the GP has any concerns or uncertainty as to the optimal approach (Box 2). Patients in some rural or remote locations may have access to relevant specialists via telehealth services. Although MDT assessment is highly recommended, in situations where access may be limited, referral to a respiratory physician or thoracic surgeon for further assessment should be considered.
{kind=link}
Cancer Australia’s Optimal Care Pathway for People with Lung Cancer recommends that the first specialist appointment should take place within two weeks of the initial GP referral, although it is not entirely clear how this applies to indeterminate nodules.23 This referral period may be anxiety-provoking as patients tend to overestimate their risk of lung cancer.24 GPs play an important role in offering reassurance and managing expectations of those with a low probability of malignancy, and providing sufficient information to alleviate anxiety in those awaiting specialist assessment. In a quality improvement initiative, a pulmonary nodule factsheet for either incidental or screening-detected nodules was found to significantly reduce anxiety and improve understanding of the circumstances.25
After the initial consultation with a specialist, it is expected that any diagnostic investigations be completed within two weeks.23 For patients with suspected or confirmed cancer, MDT discussion is essential to not only develop a treatment plan, but to establish patient links with specialist lung cancer nurses and care coordinators who provide vital support to patients. GPs continue to be essential in shared or team care arrangements with the patient and family.
The importance of multidisciplinary team assessment
Given the rapidly changing landscape for investigation of indeterminate nodules and treatment of early stage lung cancer, a comprehensive, expert lung cancer MDT assessment is now considered essential to ensure consistent, evidence-based high-quality care for patients and to avoid unnecessary procedures and related complications.7,26 A recent Australia-wide study reported widespread variation in provision of lung cancer MDT care, and a recent report from Victoria showed that up to 40% of new lung cancer cases were not discussed at a specialist MDT, with a clear survival benefit for those cases that were discussed.26,27 There is a need for healthcare professionals, patients and families to press for cultural change from institutions to ensure best evidence-based practice is provided for every lung cancer patient in Australia.
The Optimal Care Pathway for People with Lung Cancer specifies MDT membership should include a ‘core’ team, who attend all or most meetings either in person or remotely, as well as an extended team.23 Integrated smoking cessation as part of nodule management is critical.28 The evidence-base to support the requirement for lung cancer MDT-based care is clear: multiple studies have shown improved overall survival at two, three and five years, lower 30-day mortality after resected non-small cell lung cancer (NSCLC), better accuracy of staging, higher pathological confirmation rates and higher rates of receipt of curative (any tumour-specific) treatment for NSCLC.27,29-33
Decisions regarding tissue diagnosis for sub-centimetre nodules are challenging and there is occasionally a role for primary surgical resection or stereotactic radiotherapy without a tissue diagnosis. Such a decision needs to be balanced against the need for tissue to facilitate molecular mutation analysis.26 Minimally invasive video-assisted thoracic surgery is now the gold standard, with fewer complications, better global health status and similar oncologic outcomes compared with open thoracotomy.7 Further, the role of radiotherapy and immunotherapy in early stage NSCLC is evolving rapidly.26 For all of these reasons, a comprehensive, patient-centred MDT review for any patient with potential early-stage NSCLC is now an essential component of high-quality, patient-centred care.
Lung cancer screening programs
There is a clear mortality benefit to screening high-risk individuals using low-dose CT (LDCT) as part of dedicated screening programs.2,3 Early lung cancer detection leads to a stage shift and better outcomes: patients diagnosed with stage 1A lung cancer have a greater than 75% five-year survival rate, compared with less than 5% at stage 4.34 International uptake of screening programs has been slow and, at this time, there is no formal Australia lung cancer screening program. However, under direction from the Federal Government, Cancer Australia is currently investigating the possibility of an Australian lung cancer screening program (LCSP).35
A key foundation of any population-based screening program is that it must minimise harm to individuals. Therefore, one of the crucial areas for a successful and safe LCSP is the correct and optimal management of screen-detected nodules to avoid harm from unnecessary and inappropriate interventions.
Detection of pulmonary nodules through LCSPs
The reported prevalence of pulmonary nodules in screening programs varies depending on study-related factors (e.g. the definition of a nodule) and geographic location (e.g. where endemic infections like tuberculosis and coccidioidomycosis may result in nodules as part of the healing process).2,36,37 These factors partly explain the range of reported nodule prevalence from large studies, such as 13 to 24% in UK studies, about 20% in North American studies and over 50% in the Dutch-Belgian lung cancer screening trial (NELSON study), which used a volume-based definition for a nodule.3
In Australia, the Queensland Lung Cancer Screening Study found that 50% of participants at baseline had an indeterminate pulmonary nodule (using greater than 4 mm as the definition). An early analysis of the Australian-based International Lung Screening Trial (ILST) reported that 43% of baseline scans showed a pulmonary nodule.38,39 The prevalence and intensity of smoking within a study population may also influence nodule prevalence, with pulmonary nodules found in just 10% of participants in the Western Australian Asbestos Review Program, consisting of a population all exposed to asbestos but with one-third never-smokers and a modest median exposure of 19 pack-years in the ever-smokers.40
Evaluation of pulmonary nodules detected in LCSPs
Objective synoptic reports are essential for any screening program and properly accredited centres are needed to provide standardised and consistent reporting methods to inform nodule management. In the USA, the Lung Imaging Reporting and Data System (Lung-RADS) is most widely used, categorising nodules by morphology, size and growth patterns, and providing clinicians with suggested intervals for repeat imaging or intervention.15 The Lung-RADS is mostly derived from a consensus-based approach, and, although likely a safe clinical approach, adherence is variable and it may not be the most efficient approach when compared with other statistical, risk-based approaches.39,41
The Brock University cancer prediction equation (or PanCan model) is a predictive tool for the probability of a screening-detected nodule being malignant. The model was derived and validated in North American study populations and uses variables from the individual and the nodule itself to yield a percentage risk of that nodule being malignant (Table).6 The exact risk thresholds to guide management are not known and the ILST study has prospectively evaluated the safety and effectiveness of the Brock University cancer prediction equation, with initial results suggesting that this approach identifies a similar number of high-risk nodules when compared to LungRADS and safely categorises lower-risk nodules to a longer follow up interval.39 This will result in fewer CT scans being performed, with less cost to the overall program and less potential harm to participants. In Australia, it is highly likely that a future screening program will adopt the Brock University cancer prediction equation for informing management of indeterminate nodules.35
There has been considerable discussion with stakeholders, including GPs, regarding the proposed role(s) for GPs within a possible LCSP in Australia. Although project plans are not finalised, it is likely that GPs will not be leading the management of screening-detected nodules. This will be managed within the LCSP as part of the reporting process after the LDCT scan. However, GPs are likely to play a crucial role in the recruitment process for participants in any future LCSP and may be central in coordinating the management of incidental findings from the LDCT scans.
Conclusion
Pulmonary nodules are becoming more prevalent in general practice. Certain patient and nodule characteristics can help predict the probability of malignancy. An awareness of risk prediction models and pathways of specialist referral are important to minimise the impact of lung cancer. RMT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.