Detection of Legionnaires’ disease in general practice
Dr Williams is an Infectious Diseases and Microbiology Registrar, Austin Health, Melbourne. Dr Leroi Is the Director of Microbiology at Austin Health, Melbourne. Professor Johnson is Director of Research and Deputy Director, Department of Infectious Diseases, Austin Health, Melbourne; and Professor, Department of Microbiology and Immunology and Department of Medicine, University of Melbourne, Melbourne, Vic.
Lung diseases
Legionella is a significant cause of pneumonia and frequently causes severe disease. Owing to the association of Legionella with water and soil-borne outbreaks, detection of Legionella has implications for patient management and public health.
- Legionella is an important cause of severe pneumonia with significant mortality. Early appropriate antimicrobial therapy improves outcomes.
- Legionella has been associated with numerous outbreaks worldwide. Urgent notification to relevant public health departments in all Australian states and territories is required to allow rapid intervention by public health authorities.
- Risk factors for legionellosis include age 55 years or more, chronic lung disease, immunosuppression, smoking, recent travel and underlying medical conditions such as diabetes; however, legionellosis can occur in patients without apparent risk factors.
- Legionella pneumophila and L. longbeachae are the most commonly implicated causes of legionellosis in Australia.
- Rapid diagnosis of legionellosis can be made with urinary antigen and nucleic acid amplification testing on respiratory samples. Respiratory samples for culture are also important for diagnosis and epidemiological investigations.
Legionella was first described in 1976 when it was identified as the pathogen causing an outbreak of a febrile illness with pneumonia, associated with 221 suspected cases and 34 deaths, at an American Legion Convention in Philadelphia.1 Legionellosis has since been characterised by two distinct clinical syndromes: Legionnaires’ disease, the more common pneumonia syndrome; and Pontiac fever, an acute, influenza-like, self-limiting illness.2
Legionella species are ubiquitous in freshwater habitats, soils and potting mixes. Free-living amoebae and biofilms are the main environmental reservoirs for Legionella pneumophila. L pneumophila has co-evolved with free-living amoebae and is able to infect and replicate inside vacuoles within these freshwater parasites which consume biofilm, where L. pneumophila can also persist.3 Legionella species can grow at temperatures between 20 and 42°C.4 Legionellosis can present in sporadic or outbreak settings. L. pneumophila is ubiquitous in modern water distribution systems, with disease usually associated with man-made structures that generate aerosols, including cooling towers, spas and fountains. L. longbeachae is most commonly associated with sporadic disease following soil or potting mix exposure. Legionella species are transmitted via inhalation of aerosolised organisms from infected water, soil or potting mix. Nosocomial outbreaks have occurred; thus, Legionella can be a cause of nosocomial as well as community-acquired pneumonia. Nosocomial transmission tends to occur due to inhalation of aerosols from water distribution systems within the hospital environment and occasionally from air-conditioning cooling towers. Person-to-person transmission has not been reported.
Legionella has been associated with numerous disease outbreaks in Australia and internationally. Owing to the public health significance of this pathogen and its association with outbreaks, urgent notification is required on suspicion of the disease. In all Australian states and territories, the treating clinician must telephone the relevant public health department.
There are more than 50 species of Legionella, and about half of these are associated with human infection. L. pneumophila serogroup 1 and L. longbeachae are the most commonly implicated causes of legionellosis in Australia.5 In 2014 nationally, the rate of legionellosis was 1.8 per 100,000 people. In 54% of cases the causative species was L. pneumophila and in 45% it was L. longbeachae.5 Recent studies have shown that the clinical features of L. pneumophila and L. longbeachae infection are similar.6,7
Clinical presentation
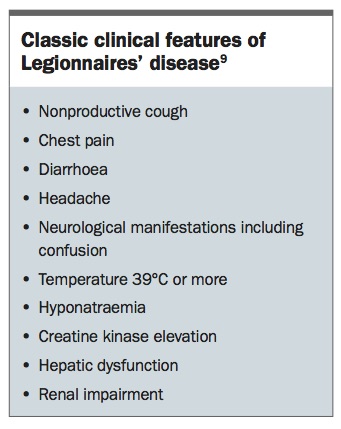
Legionella is the second most common bacterial cause of atypical pneumonia in Australia, second only to Mycoplasma pneumoniae.8 The features that characterise the clinical syndrome of Legionnaires’ disease are shown in the Box.9 Patchy infiltrates are the most commonly described chest radiographic findings, and pleural effusions are also common. Chest radiographic findings may worsen during the first week of illness despite clinical improvement.10 Legionella frequently causes severe disease. Several Australasian publications over the past decade have shown that between 40 and 60% of hospitalised patients identified with Legionella infection have required support in an intensive care unit.6,8,9 It is not possible to reliably distinguish Legionella pneumonia from other types of typical and atypical pneumonia; hence, the diagnosis should be considered in any patient with progressive or severe pneumonia.
{kind=link}
Risk factors for legionellosis include:
- age 55 years or more
- chronic lung disease
- immunosuppression
- smoking
- recent travel
- underlying medical conditions such as diabetes.
However, in a retrospective review of six clinical trials including 1551 evaluable patients, of whom 71 had documented Legionella infection, 20% did not have a history of smoking or respiratory disease and were under 55 years of age, demonstrating that Legionella pneumonia can occur in a wide range of people.11 The incubation period for legionellosis is two to 10 days. During a known outbreak, the public health department will issue an alert identifying the geographical area of suspicion. Patients who present with influenza-like symptoms and pneumonia within this incubation period and who have spent time in this area should be specifically investigated and assessed for consideration of empirical treatment for Legionella. Delays in appropriate antimicrobial therapy are associated with increased mortality.12 Early, appropriate antimicrobial therapy, contemporary intensive care practices and modern diagnostic tests have improved mortality rates from historical highs of up to 26% in 1980, to 5% or lower in more recent studies.13
Detection of legionellosis
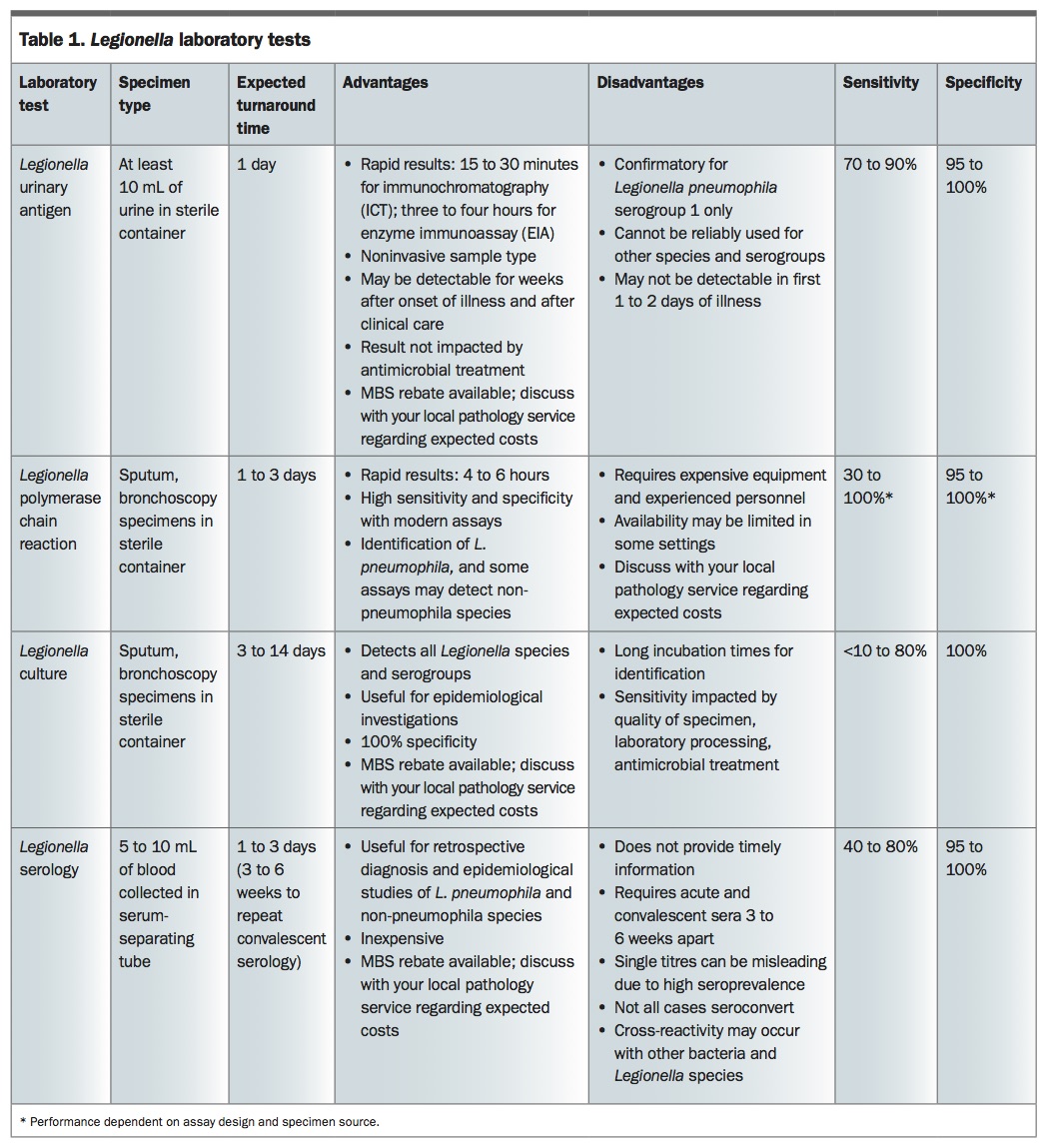
The commonly used laboratory detection methods for Legionella are described below and summarised in the Table. The main specimens for collection are an ‘on-demand’ urine sample for Legionella urinary antigen testing, lower respiratory tract samples such as sputum or bronchoscopy specimens for Legionella culture or nucleic acid amplification test (NAAT) and serum for serological testing. Patients with legionellosis will frequently not have a productive cough; however, because of the intracellular nature of this pathogen, sputum samples that do not look macroscopically purulent may still yield Legionella on culture or NAAT. Investigations for Legionella included in the MBS are Legionella urinary antigen, culture and serology. Discussion with your local pathology service regarding the expected costs for the following tests is recommended because Medicare reimbursement of pathology tests is complex and varies according to the test requested and Medicare status of the patient.
{kind=link}
Urinary antigen test
The Legionella urinary antigen test detects antigen to L. pneumophila serogroup 1 in urine immunochromatographic kits, similar to home pregnancy tests and enzyme immunosorbent assays. The Legionella urinary antigen test has a number of advantages, including ease of sample collection, simplicity of the test procedure and speed. Antigen can be detected two to three days after the appearance of clinical symptoms and may be excreted for prolonged periods, with one publication documenting detection up to 326 days after onset of infection.14 These tests may occasionally detect other Legionella species and L. pneumophila serotypes due to cross-reactivity with the L. pneumophila serogroup 1 antigen; however, they are unreliable for this use and other methods should be used for detection.4 Australian guidelines for management of community-acquired pneumonia suggest performing Legionella urinary antigen testing in all patients with severe pneumonia.15
Nucleic acid amplification test
A NAAT can be performed on lower respiratory samples. A NAAT is most commonly performed using real-time polymerase chain reaction (PCR) methods and is highly sensitive and specific for Legionella detection, with the additional benefits of rapid turnaround time and, depending on the assay, potential detection of non-L. pneumophila species.4 Commercial and in-house-developed NAATs are available in many clinical laboratories in Australia. Multiplex atypical pneumonia PCR panels that detect Legionella species as well as a number of other atypical pneumonia pathogens may be performed within your local pathology service, or samples may be sent to a reference laboratory for a NAAT for Legionella species.
Culture
Despite its ability to survive well in aquatic environments, Legionella is difficult to isolate in the laboratory as it is a fastidious, Gram-negative organism that requires a number of growth factors for adequate isolation. Legionella can be identified as early as day three with specialised culture media but may take up to seven days to grow; some non-pneumophila species may require prolonged incubation for up to 14 days.4 Most laboratories will not perform routine Legionella culture on all lower respiratory tract samples, therefore a Legionella culture should be specifically requested if the diagnosis is suspected. Isolation of Legionella species by culture is the gold standard for Legionella diagnosis; however, culture sensitivity depends on the quality of the specimen, because the presence of contaminant microorganisms and antibiotic therapy reduces the yield.4 Importantly, a negative culture does not exclude the diagnosis of legionellosis.
Serology
Detection of legionellosis via serological testing is used less frequently due to the increased availability of more rapidly available diagnostic methods. A serological diagnosis of legionellosis can be made by detection of seroconversion or a fourfold rise in serum antibody titre between acute and convalescent samples. Convalescent samples should be taken three to six weeks after onset of illness. A single high antibody titre level (1:512 or more) to L. pneumophila or L. longbeachae is suggestive of legionellosis in the correct clinical context; however, antibodies can also be detected in up to about 30% of healthy people.4 The specificity of serology for non-Legionella pneumophila serogroup 1 species is variable due to cross-reactions among Legionella species and other bacteria.
Clinical management
Appropriate early clinical management of patients with suspected legionellosis is imperative, as delayed antimicrobial therapy is associated with increased mortality.12 In practice, empirical treatment of community-acquired pneumonia is required, with the Australian therapeutic guidelines providing recommendations regarding appropriate management, including the use of pneumonia severity scores such as SMART-COP and CURB-65 to categorise patient presentations into mild, moderate and severe pneumonia (Flowchart).15-18
Due to the intracellular location of Legionella, optimal antimicrobial therapy is with agents that achieve high intracellular concentrations such as macrolides, fluoroquinolones, tetracyclines and rifampicin. In contrast, beta-lactam antibiotics such as amoxicillin and cefalexin are inactive. The Australian therapeutic guidelines recommend treatment with azithromycin 500 mg daily for five to seven days or doxycycline 100 mg, 12 hourly for 14 days in mild-to-moderate legionellosis. Patients with severe legionellosis should be managed with intravenous azithromycin in the acute hospital setting and referred for specialty involvement.18 Detection of Legionella by culture, PCR or a single antibody titre of 1:512 or more requires immediate notification by telephone to the relevant state or territory public health department.
Conclusion
Legionella is an important cause of community-acquired pneumonia. The primary care physician plays a crucial role in the diagnosis and management of legionellosis, including appropriate referral for inpatient management in the setting of moderate-to-severe disease. Rapid diagnosis can inform appropriate clinical management and epidemiological investigations that may lead to preventive measures that reduce the impact of outbreaks. RMT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.