Five steps to reducing risk in community-acquired pneumonia

Dr Abbott is a Respiratory Physician in the Department of Respiratory Medicine, Nepean Hospital, Sydney; and Clinical Lecturer in the Nepean Clinical School, The University of Sydney. Dr Morgan is Senior Physician in the Department of Respiratory Medicine, Concord Hospital and Nepean Hospital, Sydney; Associate Professor in The University of Sydney School of Medicine, Sydney, NSW; and Chair of the Lung Foundation Australia Respiratory Infectious Diseases Group.
Lung diseases
Community-acquired pneumonia (CAP) causes significant morbidity and mortality, particularly among older people and those with chronic disease. We propose a five-point strategy to reduce the risk of CAP, consequent hospitalisation and complications. It includes pneumococcal and influenza vaccinations, minimisation of inhaled corticosteroids, smoking cessation, alcohol reduction and antiplatelet therapy after CAP.
- Community-acquired pneumonia (CAP) is common and causes significant morbidity and mortality, particularly among older people and those with chronic illness.
- Vaccination against the most common causes of CAP, Streptococcus pneumoniae and influenza virus, reduces CAP incidence substantially.
- Smoking and alcohol abuse are important risk factors for CAP, and smoking and alcohol harm minimisation strategies are recommended whenever possible.
- Inhaled corticosteroids may increase CAP risk in patients with chronic obstructive pulmonary disease and should be used only in those who meet local guideline criteria.
- Evidence is increasing for an association between CAP and cardiovascular events; a course of aspirin should be considered in all patients after CAP.
Respiratory tract infections are a common reason for GP consultation. Community-acquired pneumonia (CAP) – the combination of symptoms of a lower respiratory tract infection and demonstration of pulmonary parenchymal involvement on imaging – accounts for about one in every 1000 GP consultations in Australia.1 Hospital admissions increase dramatically for patients with CAP aged over 60 years. Among patients with CAP admitted to hospital, almost 10% require intensive care support, and 8% of these patients die.2
There are many risk factors for CAP (Box 1). Among the most important are cigarette smoking, airways disease, alcohol dependence, older age and chronic medical illness.3-5 The presence of multiple risk factors (risk stacking) in patients with pneumococcal pneumonia is associated with a poorer prognosis, poorer tolerability of treatments and increased admissions to hospital, with an increased risk of further complications.6,7 The use of inhaled corticosteroids, often prescribed as a treatment for chronic obstructive pulmonary disease (COPD) and asthma, is also a risk factor.8 Further, pneumonia is a risk factor for acute cardiovascular events in the short term, and is associated with increased mortality among survivors in the long term.9
{kind=link}
In this article, we discuss a five-point strategy that can be implemented in primary care to reduce the risk of CAP and its complications.
Vaccination
The most common causes of CAP in Australia remain Streptococcus pneumoniae and influenza viruses (Box 2). Federally funded programs are in place to support both pneumococcal and influenza vaccinations.
{kind=link}
Pneumococcal vaccination
Globally, S. pneumoniae infections are the major cause of fatal respiratory infections across all age groups.10 In Australia, S. pneumoniae is responsible for 20% of pneumonia cases.11 Two types of pneumococcal vaccine are available: polysaccharide and conjugate vaccines.
Pneumococcal polysaccharide vaccine
The 23-valent pneumococcal polysaccharide vaccine (23vPPV), containing the 23 capsular types of S. pneumoniae that are responsible for most cases of invasive pneumococcal disease (IPD) in adults in Australia, is currently provided free under the National Immunisation Program Schedule to those at greatest risk for pneumococcal pneumonia (www.immunise.health.gov.au). These include people aged 65 years and over, Indigenous Australians aged 50 years and over, Indigenous Australians aged 15 to 49 years who are medically at risk, and infants under 12 months. A second dose of vaccine is also available to Australians with immunocompromising conditions or chronic disease and to smokers, a minimum of five years after their first dose.
The vaccine is also available on the PBS for all adults aged 18 years or over who are smokers or medically at risk, such as those with chronic lung, heart or liver disease or diabetes. People younger than 65 years with another risk factor are also likely to benefit from vaccination and are encouraged to purchase 23vPPV.
There have been changes to the TGA-approved revaccination schedule over recent years. The second dose of 23vPPV in otherwise healthy people aged 65 years and older was removed in 2011 because of concerns about adverse reactions and doubts about the net benefit of this dose.12
Pneumococcal conjugate vaccines
Pneumococcal conjugate vaccines (PCVs) are the backbone of the funded Australian paediatric vaccination program. Currently, a 13-valent PCV (13vPCV) is recommended for all infants and children. For adults, it is recommended (but not funded) only for those with immunocompromising conditions.
Impact and uptake of pneumococcal vaccination
Pneumococcal vaccination has been highly effective in reducing the global morbidity and mortality of IPD, but until recently the evidence of its benefit against pneumonia has been less clear, relying on observational studies.13,14 However, the recent Netherlands Community-Acquired Pneumonia Immunization Trial in Adults (CAPITA) is the first randomised controlled trial to show that use of PCV in adults leads to a reduction in CAP caused by vaccine-type pneumococci.15 This has led to the licensing of 13vPCV for adults as well as children in Australia. The Pharmaceutical Benefits Advisory Committee has recommended funding 13vPCV for people aged 65 years and over, to replace 23vPPV, but this has yet not been implemented. The cost-effectiveness of 13vPCV is currently under review.
The paediatric vaccination programs have been highly effective in reducing pneumococcal disease in children. The high vaccine uptake in children has helped their parents and particularly grandparents, with herd immunity contributing to the decline in rates of IPD and noninvasive pneumococcal disease caused by serotypes covered by the childhood 13vPCV.16 Some serotypes in circulation are not covered by either vaccine type.
Several observational studies have found 23vPPV to be effective against CAP caused by vaccine types, reporting up to 48% vaccine efficacy against pneumococcal CAP and 25% against all-cause CAP.13,14 So, although the vaccine efficacy of 23vPPV remains imperfect, there is evidence of its benefit in adults, especially when 23vPPV uptake is high. This is particularly relevant in Australia, where adult pneumococcal vaccination rates have been falling steadily. Despite about 93% pneumococcal vaccination coverage for children, coverage for adults has fallen to 47% in NSW.17 The reasons for this fall are likely multifactorial. However, as the fall appears to have started around the time of the change to the schedule for a second dose of 23vPPV, it may reflect patients and doctors losing confidence in the vaccine.
Uptake is lower for pneumococcal vaccination than for influenza vaccination. Anecdotally, both patients and clinicians have been reluctant to give the two vaccines on the same occasion. Scheduling a return visit is problematic for all. It is safe to give pneumococcal vaccine and influenza vaccine on the same day. An opportunistic, ‘while you are here …’ approach from GPs might help increase vaccine coverage.
Influenza vaccination
Influenza vaccination is clearly effective in reducing seasonal influenzal illness, but relatively few studies have shown a reduction in postinfluenza complications such as CAP. The US Centers for Disease Control and Prevention Etiology of Pneumonia in the Community (EPIC) study is a prospective multicentre study in 2767 children and adults that assessed the association between influenza vaccination status and hospitalisation for community-acquired laboratory-confirmed influenza pneumonia. Assuming a vaccine effectiveness of about 56%, influenza vaccination more than halved the risk of developing pneumonia.18
Antiplatelet therapy
There is increasing evidence for an association between CAP and acute and longer term cardiovascular events. Systematic reviews of observational studies show that about 18 to 30% of patients hospitalised for CAP experience a cardiovascular complication in the 30 days after diagnosis, with 5% having acute coronary syndrome.19,20
Further, a recently reported study linking the Scottish Morbidity Record with national infection surveillance data identified adults with a first myocardial infarction or stroke between 2004 and 2014 and laboratory-confirmed cases of respiratory infection during the same period. Myocardial infarction rates were substantially increased in the week after S. pneumoniae and influenza virus infections. Rates of stroke were also high after S. pneumoniae and influenza infection and remained elevated to 28 days.21
Cardiovascular complications are the key factors in increased long-term mortality of survivors of CAP and a reduction in survival that is seen out to 10 years. Although the presence of cardiovascular disease is a risk factor for further events post-CAP, the increased risk is also seen in patients without previously known cardiovascular disease.19,22
Several mechanisms have been proposed for the increase in cardiovascular events after CAP:20
- Inflammation induces a procoagulant state and increases the risk of thrombosis in a critically narrowed vessel.
- Inflammation destabilises atheromatous plaques and increases the risk of acute plaque rupture.
- Pneumonia increases heart rate and myocardial oxygen consumption, resulting in a vulnerable myocardium exposed to reduced filling time.
- Some causes of pneumonia (influenza virus and S. pneumoniae) can cause a direct myocarditis and consequent fibrosis.
Observational data suggest that statins, ACE inhibitors and antiplatelet agents may all help reduce cardiovascular complications post-CAP.20 A randomised controlled trial examining the role of aspirin in preventing acute coronary syndrome after pneumonia found that aspirin at a dose of 300 mg daily for one month post-CAP was associated with a significant (9%) reduction in acute coronary syndrome and cardiovascular death.23 There is a lack of high-level evidence to support the benefit of a longer duration of therapy but further trials are awaited.
The benefits of aspirin for primary prevention of cardiovascular disease are clear. After CAP, a course of aspirin (300 mg daily for a month) should be considered even in patients with no other cardiovascular risk factors.
Corticosteroid minimisation
Inhaled corticosteroids are a cornerstone of treatment for patients with asthma. They are also widely prescribed for patients with other chronic airway diseases, such as COPD and bronchiectasis. This is despite their benefit having been shown only in patients with more severe COPD with recurrent exacerbations and little evidence of their benefit in patients with bronchiectasis. Pneumonia is more common with increasing age and in patients with chronic disease, but there is evidence that high doses of inhaled corticosteroids are associated with a higher risk of pneumonia in patients with COPD.8 The same pneumonia risk does not seem to exist when inhaled corticosteroids are used in asthma.
Guidelines from Lung Foundation Australia recommend a stepwise approach to the management of COPD. In this approach, inhaled corticosteroids and long-acting beta-adrenoceptor agonists can be considered for patients with COPD who have a forced expiratory volume in one second less than 50% predicted and a history of frequent exacerbations (two or more in the previous 12 months).24 Withdrawing inhaled corticosteroids from patients who do not meet these criteria appears safe and reduces the risk of pneumonia substantially.25,26
Smoking cessation
Although smoking rates in Australia have fallen significantly over the past decade, more than one in seven adults (2.6 million people) currently smoke tobacco daily. Proportionally, more men (16.9%) smoke than women (12.1%).27
There is consistent evidence that smoking is associated with an increased risk of CAP. In a Spanish population-based case-control study that captured both CAP managed in hospital and CAP managed in the community, being an ever-smoker increased the risk of developing CAP compared with never-smokers (odds ratio [OR], 2).28 The authors estimated that one in three cases of pneumonia in adults would have been avoided if no-one in the population smoked.
A North American study investigating the relationship between cigarette smoking and IPD found smoking to be the strongest independent risk factor for IPD among immunocompetent, nonelderly adults (OR, 4).29 There were dose-response relations with IPD for current number of cigarettes smoked, pack-years of smoking and time since quitting.29
Current smoking increases the severity of pneumococcal pneumonia and the risk of death.30 It impairs humoral and cell-mediated defence mechanisms, reduces mucociliary clearance and facilitates adhesion and invasion of pathogenic organisms.
Smoking cessation has immediate and long-term health benefits. However, despite clear links between smoking and CAP there is less evidence of the benefit of smoking cessation in reducing future risk of CAP. Although one study suggested that former smokers had a 50% reduction in their risk of CAP five years after smoking cessation, another suggested it might take 10 years to see a benefit and this benefit might be attenuated in patients who have already developed COPD.28,31
A hospital admission often presents an opportunity for patients to quit smoking as they usually reduce or cease their cigarette use, partly because they feel unwell and partly because smoking is not permitted in hospitals. The postdischarge review is an opportune time for GPs to talk with patients about long-term cessation. However, there is never a bad time to discuss smoking cessation. Even a brief intervention (e.g. the 5 As – ask about smoking, advise quitting, assess current willingness to quit, assist in the quit attempt and arrange timely follow up) can improve the frequency and success of any quit attempt.32,33
Alcohol reduction
Daily alcohol consumption of more than 40 g (four standard drinks) is a dose-dependent risk factor for pneumonia. This risk is cumulative in combination with current smoking.
Compared with zero alcohol consumption, consumption of up to 40 g alcohol daily appears to have no significant effect on risk of CAP. However, the risk of CAP increases linearly for those who drink more than this.5 Alcoholism is associated with an eightfold increased risk of CAP.34
Asking about daily alcohol intake and recommending reducing to the level recommended by current Australian guidelines for healthy men and women (less than 20g or two standard drinks daily) offers significant reduction in risk of CAP.35
Summary
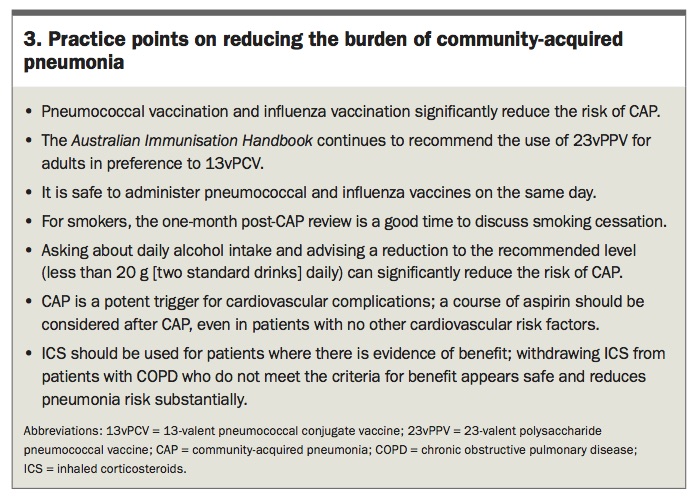
Smoking and alcohol abuse are preventable risk factors for pneumonia, and much can be gained from implementing smoking and alcohol harm minimisation strategies. In addition, introducing an appropriate pneumococcal vaccination schedule, reducing viral infections such as influenza, treating underlying diseases such as COPD according to local evidence-based guidelines and considering antiplatelet treatments to reduce post-CAP complications have potential for benefit. Practice points on these strategies to reduce the burden of CAP are shown in Box 3. These strategies set a path to significantly reducing the risk of patients developing CAP and its complications. RMT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.